Accessibility of Mainstream Services for Aboriginal Victorians
Overview
The Victorian Aboriginal population was around 47 000 at the 2011 census, making up around 0.9 per cent of the overall population. Aboriginal Victorians experience considerable disadvantage compared to the non-Aboriginal population, with higher perinatal mortality, higher disability rates and lower literacy and numeracy outcomes.
The Victorian Aboriginal Affairs Framework 2013–18 (VAAF) outlines criteria to apply to service design and delivery to ensure that services are accessible, and a set of targets relating to closing the gaps and ensuring that Aboriginal Victorians receive equitable access to mainstream services.
This audit assessed the accessibility of mainstream services such as hospitals, maternal and child health services, schools and kindergartens, and community and public housing for Aboriginal Victorians.
The audit found little improvement in outcomes, and in some cases, the gap has worsened. However, access to hospitals, maternal and child health services, housing services and kindergarten has improved. An absence of effective leadership and oversight has affected mainstream service delivery over many years. The Secretaries’ Leadership Group on Aboriginal Affairs is responsible for overseeing implementation of VAAF and has not been effective. Without strengthened oversight and improved collaboration between departments, VAAF will not be implemented effectively and its intended outcomes are not likely to be achieved.
Accessibility of Mainstream Services for Aboriginal Victorians: Message
Ordered to be printed
VICTORIAN GOVERNMENT PRINTER May 2014
PP No 325, Session 2010–14
President
Legislative Council
Parliament House
Melbourne
Speaker
Legislative Assembly
Parliament House
Melbourne
Dear Presiding Officers
Under the provisions of section 16AB of the Audit Act 1994, I transmit my report on the audit Accessibility of Mainstream Services for Aboriginal Victorians.
The audit examined the access to mainstream services for Aboriginal Victorians that are provided or funded by government departments, and it assessed whether departments can demonstrate how improved access has contributed, and is expected to contribute to improved outcomes.
I found that despite departments developing programs aimed at increasing access, outcomes have not improved significantly and in some cases the gap has worsened. A lack of broad consultation and problems with data reliability mean that departments cannot be assured they understand the needs of Aboriginal Victorians.
With the exception of the Department of Health, departments do not know if the work they are undertaking is improving access, and why outcomes are not improving. As a result, departments cannot be assured they are on track to meet the targets in the Victorian Aboriginal Affairs Framework. There is a lack of effective oversight and coordination by the Secretaries' Leadership Group and the Office of Aboriginal Affairs Victoria. Without improvements in these areas, it is unlikely the Victorian Aboriginal Affairs Framework 2013–18 will be effectively implemented.
I have made eight recommendations, six targeted at the Departments of Health, Human Services, and Education and Early Childhood Development, and two targeted at the Office of Aboriginal Affairs Victoria in the Department of Premier and Cabinet.
Yours faithfully
John Doyle
Auditor-General
29 May 2014
Auditor-General's comments
 John Doyle Auditor-General |
Audit team Andrew Evans —Sector Director Peter Rorke — Team Leader Sophie Fisher — Analyst Pablo Armellino — Graduate Analyst Chris Sheard —Engagement Quality Control Reviewer |
Victoria's Aboriginal population is small relative to other parts of Australia. The 2011 census reports that there are around 47 000 Aboriginal people in Victoria — 0.9 per cent of the total Victorian population — and 55 per cent of Aboriginal Victorians are under 25 years of age, compared to 32 per cent of the non-Aboriginal population.
Despite some improvements, Aboriginal Victorians are still facing significant disadvantage compared to the rest of the Victorian population, and they access many mainstream services at lower rates than the rest of the population. Gaps persist in many areas including early childhood development, health outcomes, income and employment. Addressing these gaps is vital to improve life outcomes for Aboriginal Victorians, and ensure they receive equitable access to services they are entitled to.
This audit assessed the accessibility of mainstream services for Aboriginal Victorians, including whether departments can demonstrate how improved access has, and is expected to, improve outcomes for Aboriginal Victorians. The audit focused on whole‑of-government and departmental policies, programs and strategies, as well as outcomes, covering early childhood, health and human services.
My audit found little improvement in outcomes and in some cases, the gap between Aboriginal Victorians and the rest of the population has worsened. However, access to hospital services, maternal and child health services, public housing services and kindergarten has improved.
Many of the audit findings reflect similar issues identified in past VAGO reports and various departmental reviews relating to disadvantaged sections of the population. These groups have differing needs and challenges in accessing mainstream services. In order to ensure they receive the same opportunities as the rest of the population, departments and agencies need to be well informed about the needs of disadvantaged groups, including Aboriginal people, and target their services and programs accordingly.
In common with other whole-of-government initiatives that focus on vulnerable Victorians, there is an absence of effective leadership and oversight in Aboriginal affairs which has affected mainstream service delivery over many years. The Secretaries' Leadership Group on Aboriginal Affairs (SLG) is responsible for overseeing implementation of the Victorian Aboriginal Affairs Framework 2013–18 (VAAF), and this has not been effective. To ensure that services are accessible — and to achieve its intended outcomes — VAAF needs to be implemented with strengthened oversight and improved collaboration between departments.
I have made key recommendations for the Department of Premier and Cabinet through the SLG to provide more active leadership and direction to make sure that departments comply with the requirements of VAAF. I am pleased DPC has accepted these recommendations and the SLG has recently created a new Inter-Departmental Aboriginal Inclusion Working Group. It is important this group, the Office of Aboriginal Affairs Victoria (OAAV) and the SLG actively oversee progress in developing and implementing plans and actions to improve Aboriginal inclusion.
The report also contains a set of recommendations that apply to all government agencies that may be responsible for providing services for Aboriginal Victorians. I am confident that adopting these recommendations will assist agencies to 'close the gap', thus improving the health and wellbeing of Aboriginal Victorians.
I intend to revisit the issues that my office has identified in this report to ensure they are being appropriately addressed.
Finally, I wish to acknowledge and thank the staff of OAAV and the departments of Education and Early Childhood Development, Health and Human Services for their assistance and cooperation during this audit.
John Doyle
Auditor-General
May 2014
Audit Summary
The Australian Aboriginal population faces considerable disadvantage when compared to the non-Aboriginal population. For example, there are significant gaps in early childhood development, lower participation in maternal and child health services and kindergarten, poorer health status and shorter life expectancy, higher disability rates and comparatively lower literacy and numeracy outcomes. Despite some recent improvements, these gaps are still prevalent in Victoria.
Victoria's Aboriginal population is small relative to other parts of Australia. The 2011 census reports that there are around 47 000 Aboriginal people in Victoria — 0.9 per cent of the total Victorian population — and 55 per cent of Aboriginal Victorians are under 25 years of age, compared to 32 per cent of the non-Aboriginal population.

Victorian Aboriginal Health Service (Fitzroy). Photograph courtesy of Tobias Titz.
In November 2008, the Council of Australian Governments agreed to the National Indigenous Reform Agreement (NIRA), which commits all Australian governments to achieving specific closing the gap targets. To address its commitments under NIRA, the Victorian Government has developed the Victorian Aboriginal Affairs Framework 2013–18 (VAAF), which builds on the previous Victorian Indigenous Affairs Framework 2010–13, as the primary whole-of-government framework for Aboriginal people. VAAF outlines criteria designed to provide more effective access to services and improve outcomes for Aboriginal Victorians.
This audit examined the access to mainstream services for Aboriginal Victorians provided or funded by government departments, and it assessed whether departments can demonstrate how improved access has contributed, and is expected to contribute to improved outcomes. The audit focused on whole-of-government and departmental policies, programs, strategies and outcomes, covering early childhood, health and human services and excluding child protection and youth justice.
Conclusions
Despite departments developing programs aimed at closing the gap between the Aboriginal population and the non-Aboriginal population, there has been little improvement in outcomes, and in some cases the gap has worsened. However, there is improved service access as a result of programs such as the Aboriginal Quitline and Aboriginal Health Promotion and Chronic Care programs, and in some areas such as maternal and child health.
An absence of effective leadership and oversight has adversely affected the delivery of mainstream services for Aboriginal Victorians over many years. The Secretaries' Leadership Group on Aboriginal Affairs (SLG) is responsible for overseeing the implementation of VAAF. This arrangement does not appear to have been effective, and there is limited evidence that the SLG is fulfilling its intended role. Crucially, it appears unable to ensure that VAAF is applied as intended across government. Similarly, the Office of Aboriginal Affairs Victoria (OAAV) does not oversee departmental activities. OAAV advised it does not have the authority to direct the way departments undertake their work and sees its role as one of coordination and facilitation. There is a lack of accountability for delivery of actions because it is up to individual departments to develop and implement their own plans, with limited oversight. However, a new Interdepartmental Aboriginal Inclusion Working Group is being created to provide for regular departmental engagement and oversight of plans and associated processes.
OAAV was not able to quantify the total amount spent by the Victorian Government in relation to services for Aboriginal people, and some departments had difficulty providing complete financial information. Therefore, the total amount of funding is not clear, and the lack of complete information makes effective monitoring of expenditure problematic.
Departments have developed a range of plans, strategies and programs aimed at improving access to services for Aboriginal people. Most of these have been in place for five to 10 years and in the case of the Department of Health (DH), some for over 20 years. Since the introduction of VAAF in 2012, departments have not reviewed or updated their plans to reflect the framework's focus on addressing service access. All departments are required to complete their Aboriginal inclusion action plans by the end of August 2014. Originally, they were due to be developed by the end of 2013, and significant work remains for these plans to identify and address barriers to access to comply with VAAF criteria. The plans should also include clear target measures and milestones, and detail the requirements for monitoring, evaluating and reporting on access and outcomes.
There is significant scope for departments to improve their monitoring, evaluation and reporting of outcomes of Aboriginal service delivery strategies and programs. Except for DH, there is little evidence that departments undertake robust evaluations to assess the achievement of outcomes for Aboriginal Victorians.
Across all departments, weaknesses in the completeness and reliability of data mean that it is difficult for them to accurately measure the achievement of outcomes. This diminishes their ability to effectively monitor, evaluate and report progress on service delivery plans. While there are challenges in obtaining data on the Aboriginal population, more should be done to improve the completeness and reliability of information, including data on population levels. Without improvements to the completeness of data, departments cannot be assured that all Aboriginal Victorians who are eligible for particular services are able to access them.
A lack of effective collaboration and coordination in planning and service delivery between the departments and service providers, as well as at service delivery level between local providers, creates difficulties for Aboriginal people, who have to navigate multiple service providers to access services. SLG is tasked with coordination and collaboration between departments, but there is limited evidence this is occurring.
Findings
Oversight and leadership
A lack of effective oversight and leadership has adversely affected the delivery of mainstream services for Aboriginal Victorians. Given the deficiencies identified in this audit — such as with Aboriginal action plans and strategies, data collection and sharing, and program evaluations — there is a pressing need for SLG and OAAV to provide more active leadership, direction and oversight to ensure that departmental programs and strategies identify and address the needs of Aboriginal Victorians to facilitate increased access and improved outcomes.
Consultation and engagement
There are a number of ways in which government departments consult and engage with Aboriginal organisations and people. However, there is a lack of broad consultation, and this limits community representation and is time consuming for stakeholders who are on multiple committees.
Consistent with VAAF and Council of Australian Governments (COAG) principles, broad consultation includes engaging Aboriginal community members and organisations, as well as mainstream service providers, at all stages of program development, implementation and evaluation to ensure diverse representation.
Many organisations — including Aboriginal community controlled organisations — that provide feedback and advice to departments are directly funded by those departments, which may diminish their capacity to provide constructive feedback. There is scope for greater use of community consultation, which would strengthen overall consultation processes.
Complete and reliable data
There are challenges for the audited departments in obtaining complete and reliable data to identify needs, develop plans, evaluate programs and report outcomes — particularly data relating to population levels. Despite these challenges, DH has had data improvement processes in place for a number of years through strategies to improve identification in public hospitals. The Department of Human Services (DHS) more recently has moved to enhance data collection procedures to improve completeness and reliability of datasets particularly relating to service accessibility for Aboriginal Victorians, while the Department of Education and Early Childhood (DEECD) is improving data collection in its maternal and child health service.
There is a clear imperative for departments to improve their data collection methods and information sharing practices. Data sharing across departments is limited. Without complete and reliable data, departments cannot be assured they are meeting the service needs of Aboriginal people.
Plans, programs and strategies
All departmental secretaries have agreed to finalise Aboriginal inclusion action plans by the end of August 2014, but significant work remains for these plans to identify and address barriers to access.
Overall, the quality of the audited sample of plans and strategies for the delivery of services to Aboriginal Victorians in the audited departments was poor. They did not meet many of the better practice criteria established in government policy framework documents. Consequently, there is considerable scope for departments to improve their plans and strategies under VAAF.
Collaboration and coordination
There is a lack of effective collaboration and coordination in planning and service delivery between the departments and service providers, as well as at service delivery level between local providers, despite this being a role of SLG. The successful implementation of VAAF requires improved cross-government coordination. Feedback from Aboriginal stakeholders, community organisations, service providers, and departmental officers indicated that many problems with government services are the result of a 'siloed' approach to service delivery that can impede access to services and negatively impact outcomes. This creates difficulties as users have to navigate multiple service providers to access services.
According to its terms of reference, SLG is responsible for strengthening coordination and collaboration between departments. However, there is limited evidence this is occurring and there is considerable scope for improvement in this area.
Access to services
Both DH and DEECD measure access to programs, and can demonstrate improvements in accessibility in some services. At DH this is the case in a range of areas, while at DEECD, gaps in participation in maternal and child health and kindergarten have narrowed. However, this data needs to be viewed with caution, because longer-term trends need to be considered rather than short-term increases or decreases in participation and attendance. DHS can demonstrate increased access to public housing — although overcrowding in public housing has increased — and to homelessness services.
Evaluating outcomes
Despite the development of programs aimed at increasing access to close the gap between Aboriginal and non-Aboriginal Victorians, there has been little improvement in outcomes, and in some cases the gap has worsened.
Without effective evaluations, departments cannot be assured they have achieved or are achieving targets under VAAF. Only DH demonstrated a rigorous program of evaluation that assessed the achievement of outcomes for Aboriginal Victorians, and this has been in place for a number of years.
While DEECD and DHS undertake some evaluations, neither could demonstrate a comprehensive evaluation regime for Aboriginal programs, and it is difficult to understand how these departments can assure themselves that plans, programs and strategies are achieving positive outcomes for Aboriginal people.
Monitoring and reporting
The Victorian Government Aboriginal Affairs Report is submitted annually to the Victorian Parliament. OAAV collects information from departments to publish in the report. However, this report provides only a high-level analysis of outcomes against targets in key areas and some basic data on trends. The information is not always reliable because it depends on data provided by departments, which is of varying quality. Departments also report to COAG, on their progress towards outcomes for closing the gap between Aboriginal and non-Aboriginal Victorians.
Although departments report on results of their various programs, there is significant scope to improve public reporting on the accessibility and outcomes of mainstream services for Aboriginal Victorians.
Funding of services
Quantifying the Victorian Government's expenditure on mainstream services for Aboriginal Victorians is difficult. DEECD was not able to provide specific details on expenditure for Aboriginal Victorians in maternal and child health, and DHS was unable to provide specific funding details in relation to access of its mainstream services by Aboriginal Victorians.
Although OAAV is the central policy group for Aboriginal affairs, it was unable to provide any information on the amount of funding provided for programs related to services for Aboriginal people across Victorian Government departments.
Recommendations
That departments:
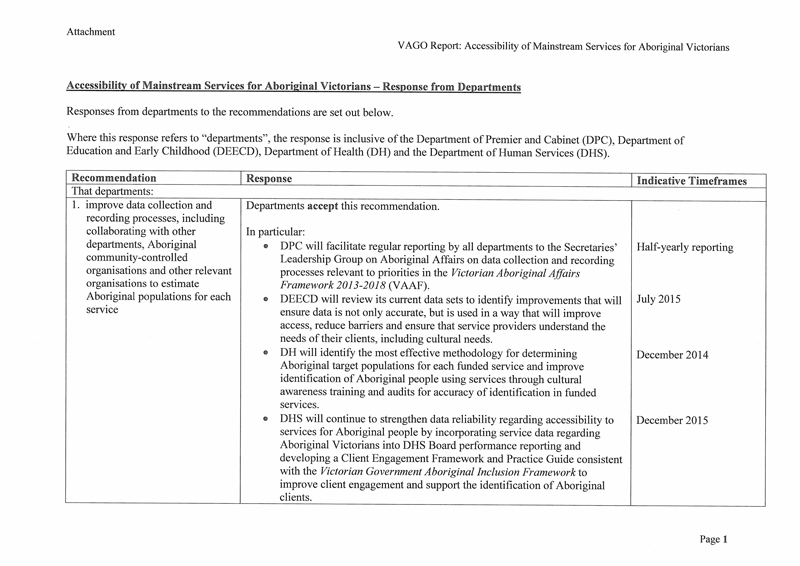
- improve data collection and recording processes, including collaborating with other departments, Aboriginal community controlled organisations and other relevant organisations to estimate Aboriginal populations for each service
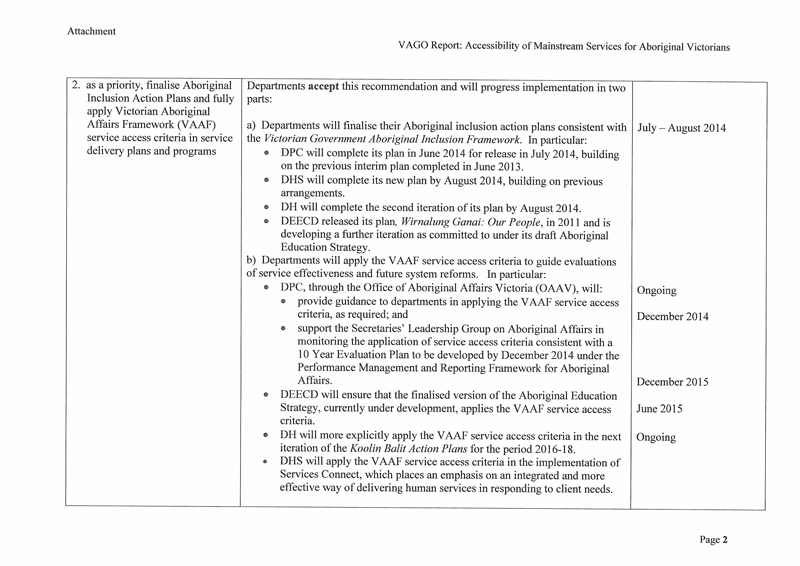
- as a priority, finalise Aboriginal inclusion action plans and fully apply Victorian Aboriginal Affairs Framework service access criteria in service delivery plans and programs
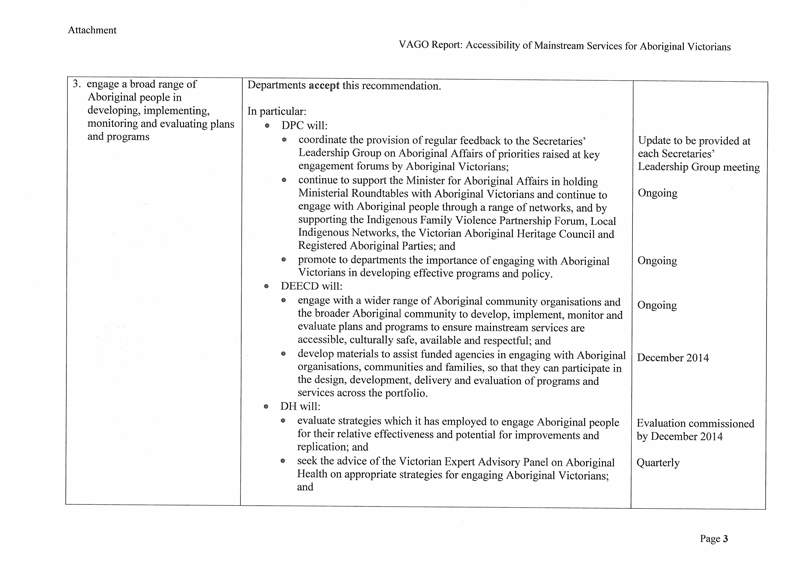
- engage a broad range of Aboriginal people in developing, implementing, monitoring and evaluating plans and programs
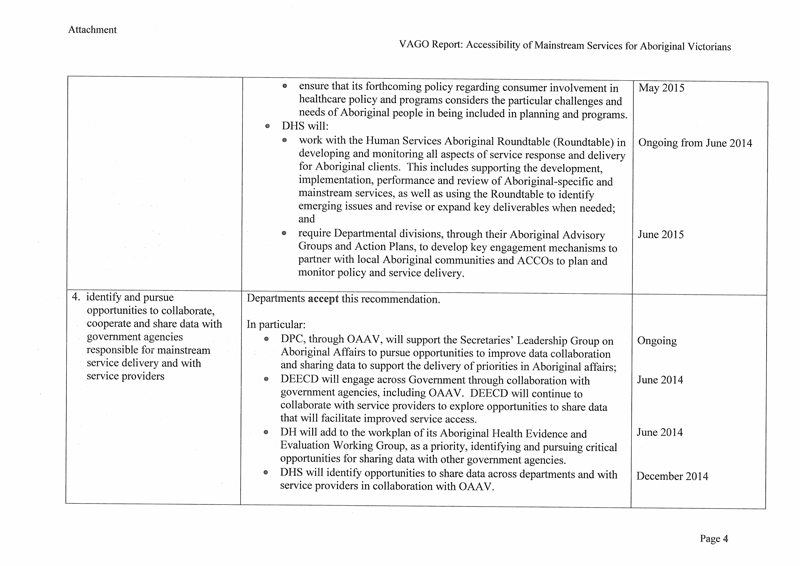
- identify and pursue opportunities to collaborate, cooperate and share data with government agencies responsible for mainstream service delivery and with service providers
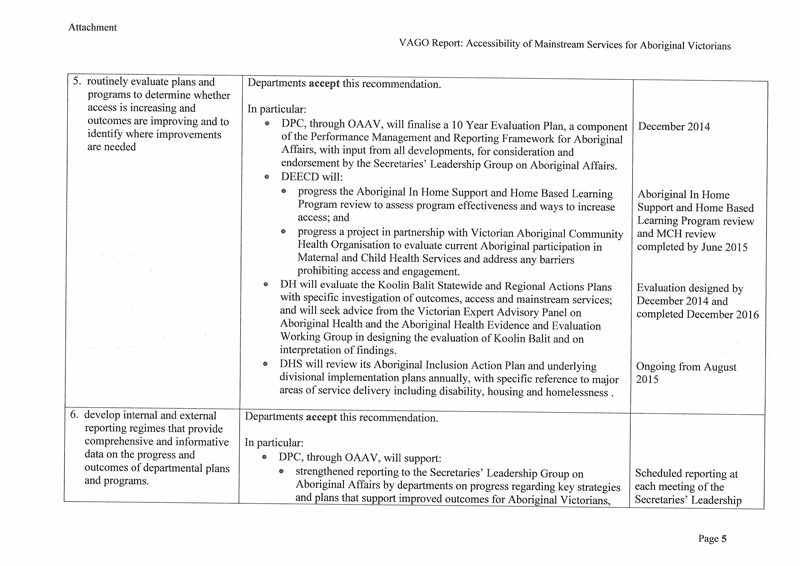
- routinely evaluate plans and programs to determine whether access is increasing and outcomes are improving, and to identify where improvements are needed
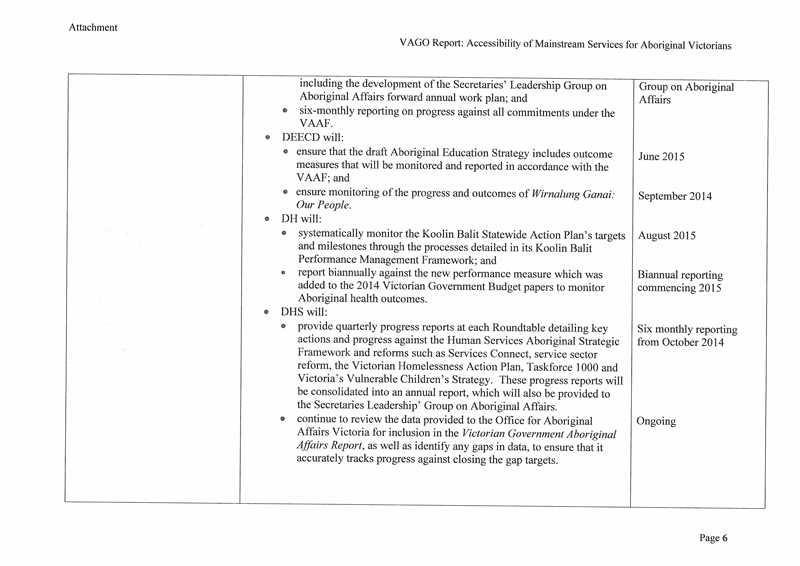
- develop internal and external reporting regimes that provide comprehensive and informative data on the progress and outcomes of departmental plans and programs.
That the Department of Premier and Cabinet:
- provides more active leadership and direction so that departmental programs and strategies comply with the Victorian Aboriginal Affairs Framework 2013–18, and identify and address increased access and improved outcomes
- through the Secretaries' Leadership Group on Aboriginal Affairs, monitors the implementation of departmental plans, evaluates outcomes and monitors the development of investment logic maps that identify the funding requirements over the term of the government's commitment to the Victorian Aboriginal Affairs Framework 2013–18.
Submissions and comments received
In addition to progressive engagement during the course of the audit, in accordance with section 16(3) of the Audit Act 1994, a copy of this report was provided to the Office of Aboriginal Affairs Victoria and the departments of Education and Early Childhood Development, Health, and Human Services with a request for submissions or comments.
Agency views have been considered in reaching our audit conclusions and are represented to the extent relevant and warranted in preparing this report. Their full section 16(3) submissions and comments are included in Appendix D.
1 Background
1.1 Introduction
1.1.1 Victoria's Aboriginal population
Victoria's Aboriginal population is relatively small compared to other parts of Australia. The 2011 census reports that there are around 47 000 Aboriginal people in Victoria — 0.9 per cent of the total population — an increase of around 40 per cent between 2006 and 2011. This growth is attributed to higher birth rates, migration to Victoria and higher rates of people identifying as Aboriginal.
The Aboriginal population is relatively young, with 55 per cent of Aboriginal Victorians under 25 years of age, compared to 32 per cent of the non-Aboriginal population. Victoria's Aboriginal population is distributed between metropolitan Melbourne — 46 per cent — and regional locations — 54 per cent.
1.1.2 Gap between the Aboriginal and non-Aboriginal population
Australia-wide
The Australian Aboriginal population faces considerable disadvantage when compared to the non-Aboriginal population — with gaps in early childhood health and development, higher than average perinatal mortality rates, lower birth weights, and lower participation in maternal and child health services and kindergarten. Aboriginal people report higher levels of psychological distress and have a poorer health status, shorter life expectancy and higher hospitalisation and disability rates. In education, comparatively lower literacy and numeracy outcomes, and higher disengagement rates, contribute to lower rates of Year 12 completion and tertiary education access.
The Victorian experience
Despite some improvements, Aboriginal Victorians are still facing significant disadvantage compared to the rest of the Victorian population. There is a gap in health and educational outcomes and therefore life outcomes between Aboriginal and non‑Aboriginal Victorians. The Council of Australian Governments (COAG) and the Victorian Government have recognised the importance of addressing Aboriginal disadvantage and closing the gap in outcomes.
Data from the 2011 census indicates that the median age of Aboriginal Victorians is 22 years, 15 years younger than the median age of non-Aboriginal Victorians. The data shows higher birth rates and a much shorter life expectancy for Aboriginal people Australia-wide. The Australian Bureau of Statistics is not able to calculate specific Victorian life expectancy rates at present because of the small size of the Victorian Aboriginal population. A large gap in median weekly income is also reported — $390 for Aboriginal and $562 for non-Aboriginal Victorians.
1.1.3 Policy framework
National Indigenous Reform Agreement (Closing the Gap)
In December 2007, COAG created a partnership between all levels of government to address Aboriginal disadvantage and close the gap between the Aboriginal and non‑Aboriginal population. In November 2008, COAG agreed to the National Indigenous Reform Agreement (NIRA), which commits all Australian governments to achieving the six Closing the Gap targets:
- close the life-expectancy gap within a generation
- halve the gap in mortality rates for Indigenous children under five within a decade
- ensure access to early childhood education for all Indigenous four-year-olds in remote communities within five years
- halve the gap in reading, writing and numeracy achievements for children within a decade
- halve the gap in Indigenous Year 12 achievement by 2020
- halve the gap in employment outcomes within a decade.
NIRA sets out an integrated strategy, which defines responsibilities, promotes accountability, clarifies funding arrangements, and links to other initiatives contributing to closing the gap. The agreement also identifies strategic areas for policies and sets out policy principles, objectives and performance indicators.
Victorian Government Aboriginal Inclusion Framework
The Victorian Government Aboriginal Inclusion Framework was released in November 2011. It outlines a number of important actions that should shape Aboriginal affairs policy. One of the key actions is to develop departmental action plans to demonstrate how access to and inclusion in mainstream services will be improved. The framework 'is designed to be flexible in its implementation and departments and agencies will be encouraged to develop their own plans, structures and strategies that suit the context within which they operate'. It is intended to provide a tool to assist departments to develop their action plans.
The framework outlines the main barriers Aboriginal Victorians face in accessing services and resources. The main barriers are actual and perceived discrimination by service providers, language and cultural barriers, lack of trust in services and organisations, and lack of awareness of and engagement with local Aboriginal communities.
Victorian Indigenous Affairs Framework
First released in 2006, the Victorian Indigenous Affairs Framework (VIAF) focused on Aboriginal childhood and early development, home environments, economic sustainability, justice, and cultural identity. All government departments were required to prepare Aboriginal Strategic Action Plans addressing key action areas and focusing on interdepartmental collaboration.
VIAF operated between 2006 and 2012. It was revised in 2010 to produce VIAF 2010‑13, which established Victorian-specific objectives and targets consistent with the nationally agreed Closing the Gap targets for 2013, 2018 and 2023. The 2013 targets were not reported against.
Victorian Aboriginal Affairs Framework 2013–18
In November 2012, the government released the Victorian Aboriginal Affairs Framework 2013–18 (VAAF) which builds on the previous VIAF as the primary whole‑of-government framework related to Aboriginal affairs. It identifies six strategic action areas, covering early childhood, education, economic participation, health and wellbeing, safe families and justice outcomes, and strong culture and confident communities. Each strategic area includes sub-objectives with specific improvement targets and expected outcomes.
Many of the indicators under VIAF related to service access and participation and are similar to the VAAF indicators and targets — for example, in action areas such as improving maternal and early childhood health, and developing and improving education outcomes.
VAAF requires all Victorian Government departments to have an Aboriginal inclusion action plan consistent with the Victorian Government Aboriginal Inclusion Framework.

Photograph courtesy of Tobias Titz.
1.1.4 Access to services for Aboriginal people
Many services that Aboriginal people need are delivered by mainstream service providers, including hospitals, maternal and child health services, schools and kindergartens, and community and public housing. The general population is entitled to access these mainstream services.
In addition, Aboriginal community controlled organisations (ACCO) provide a range of services for Aboriginal Victorians, including mainstream services such as maternal and child health, and more targeted services such as the Aboriginal Health Promotion and Chronic Care program (AHPACC), funded by the Department of Health. In many cases, these services exist to facilitate improved access to mainstream services. VAAF outlines that a significant number of Aboriginal people — 40 per cent nationally — rely on ACCO‑delivered services in areas such as health, child and family services, housing and justice.
VAAF emphasises increasing take-up of services as the first step towards improved outcomes for Aboriginal Victorians. It states that 'the challenge for service providers is to encourage or ensure that those targeted by a service actually use it'. In this context, VAAF outlines seven criteria designed to provide better access to services for Aboriginal Victorians and improve outcomes consistent with VAAF priorities. The seven access criteria are listed in Figure 1A.
Figure 1A
Key access criteria for effective service design
|
Criteria |
Outcome |
|---|---|
|
Cultural safety |
Service provider understands client needs, including cultural needs |
|
Affordability |
Clients can afford to use required services |
|
Convenience |
Clients can get to the service easily |
|
Awareness |
Current and potential clients are informed about the availability of the service and its value |
|
Empowerment |
Current and potential clients know which services they are entitled to seek |
|
Availability |
Services that a client needs are accessible |
|
Respect |
Service provider treats the client with respect |
Note: Cultural safety refers to an environment in which people feel safe, that they are respected for who they are and what they need, and that their cultural identity is unchallenged.
Source: Victorian Auditor-General's Office from the Victorian Aboriginal Affairs Framework 2013–18
VAAF recognises that more than any other state or territory, Aboriginal people in Victoria have been directly affected by the Stolen Generation. The Stolen Generation still has a significant impact on the way Aboriginal people feel about mainstream services and the level of trust they have in services that were once used as government instruments for removing Aboriginal children from their families. Also, evidence indicates that historically, Aboriginal Victorians have been excluded or discriminated against when trying to access mainstream services.
To achieve the highest level of service effectiveness, people first need to use the service, which is not an automatic decision. People consider a range of factors in making this choice. The most important challenge for all service providers, when developing a program of services designed to achieve an outcome, is making sure the intended users actually access the services.
In Victoria, mainstream services play a key role in providing health, education and welfare services to Aboriginal people, as the Aboriginal population is quite small and widely dispersed throughout the state.
According to a 2009 report by the Department of Education and Early Childhood Development (DEECD), nearly a quarter of young Aboriginal people and adults had problems accessing services. Long waits, cost and the service not being available when required were the major reported barriers to accessing services. Lack of adequate transport and distance were also commonly reported barriers.
At the 2010 Young Koori Parents Forum, organised by the Victorian Indigenous Youth Advisory Council, young Aboriginal people, particularly young parents, reported limited knowledge of services available to them, which negatively impacts the accessibility of services.
1.1.5 Identified barriers to access
Following our review of documentation — including plans, strategies and evaluation reports — and discussions with audited departments, Aboriginal stakeholders and service providers, we identified the main barriers to accessing mainstream services experienced by Aboriginal people. These include a lack of culturally safe services and a lack of awareness of the services available, racism, shame and fear, complex administrative processes and affordability. Appendix A provides further details on barriers to access and required actions.
1.1.6 Roles and responsibilities
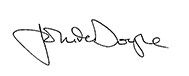
Figure 1B sets out the roles and responsibilities for the development and implementation of Aboriginal affairs policy.
Figure 1B
Roles and responsibilities–Aboriginal affairs policy
Note: Working groups under the Overarching Indigenous Bilateral Plan Committee include the Vulnerable Children's Working Group, the Economic Development Working Group, and the Data Reform Working Group.
Source: Victorian Auditor-General's Office, based on information provided by the Office of Aboriginal Affairs Victoria.
Office of Aboriginal Affairs Victoria
The Office of Aboriginal Affairs Victoria (OAAV) was established within the former Department of Planning and Community Development in December 2012 to combine Aboriginal Affairs Victoria with the Aboriginal Affairs Taskforce. In July 2013 OAAV was transferred to the Department of Premier and Cabinet. Consistent with its business plan, OAAV takes a coordinated end-to-end approach to deliver the Victorian Government's agenda for Aboriginal policy reform, community strengthening and engagement, and cultural heritage management and protection. OAAV works with Victorian Aboriginal communities and other partners to lead the whole-of-government Aboriginal affairs reform agenda to improve the lives of Aboriginal Victorians. It is also responsible for the effective implementation of the Aboriginal Heritage Act 2006 and the Aboriginal Lands Act 1970.
Secretaries' Leadership Group on Aboriginal Affairs
The Secretary of the Department of Premier and Cabinet chairs the Secretaries' Leadership Group on Aboriginal Affairs (SLG), which has a membership comprising the secretaries of all departments. SLG has a range of responsibilities, including overseeing the implementation of VAAF and driving the development and implementation of departmental Aboriginal inclusion action plans to ensure services are accessible and inclusive for Aboriginal Victorians.
Senior Officers Group
The Executive Director of OAAV chairs a Senior Officers' Group on Aboriginal Affairs with representatives from across Victorian Government departments. Its role is to provide a forum for interdepartmental collaboration and coordination.
Government departments
Departments develop policies specific to their area and coordinate service provision for Aboriginal Victorians. Each department should have an Aboriginal inclusion action plan that guides it in developing policies and services that are culturally appropriate for Aboriginal people. In terms of departmental responsibilities:
- The Department of Health has three main focus areas, health, mental health and aged care. The department works primarily in a funding and policy capacity, funding a variety of mainstream and targeted services.
- DEECD funds kindergarten programs, the Victorian Maternal and Child Health Service, parenting services, and school and higher education.
- The Department of Human Services either directly delivers or funds community organisations to deliver child protection, out-of-home care and family services, youth justice services, disability services, housing and homelessness services, and concessions.
Aboriginal Community Controlled Organisations
ACCOs are not-for-profit organisations that provide services to Aboriginal people and are administered by the community they serve. They often run programs funded by government departments involving partnerships with mainstream service providers. Generally, their focus is on facilitating access to, and improving cultural safety of, services for Aboriginal people. Their establishment and management is community driven and largely regulated through state and Commonwealth legislation. Aboriginal community controlled health organisations are well established types of ACCOs.
1.2 Previous VAGO audits
Coordinating Services and Initiatives for Aboriginal People, June 2008
The audit examined how well services and initiatives for Aboriginal people are planned and coordinated across the Victorian public sector and specifically focused on the governance and accountability arrangements in place to facilitate and monitor the progress of VIAF.
The audit examined interdepartmental and intradepartmental arrangements, and found that lack of coordinated program design was a key area for attention. Overall, the findings indicated that the respective roles and responsibilities of the agencies involved were unclear and cross-departmental collaboration was not evident. At a department level, the audit found that the departments' action plans were incomplete, or not clear in terms of interdepartmental collaboration.
The audit also identified a lack of joint datasets for departments to monitor goal achievement, and the need for a performance monitoring framework to monitor progress.
Indigenous Education Strategies for Government Schools, June 2011
The audit examined the implementation and delivery of the Wannik education strategy. It found that the strategy had a solid planning base but the rigour was not sustained throughout the rollout of the program, resulting in poor implementation. It also found that there were no comprehensive plans covering implementation milestones and time lines, stakeholder engagement and communications, and risk management. There was insufficient information available and no reporting mechanisms that provided a picture of the overall status of the Wannik strategy.
The audit reported that DEECD was unable to demonstrate that it was effectively managing the range of risks to the strategy's success. Rather than project-managing the strategy, DEECD used a business-as-usual model with a limited accountability system.
Access to Education for Rural Students, April 2014
This audit assessed the effectiveness of DEECD's activities to ensure that Victorians in rural areas have access to a high-quality education and that outcomes for these students are maximised.
The audit concluded that DEECD has not provided access to high-quality education for all students, and while DEECD undertakes many activities that assist rural educators and students, these have not resulted in significantly improved performance. The report, however, did acknowledge that DEECD's Smarter Schools National Partnerships program for people in low socio-economic areas had improved oral language skills among Indigenous students and the capacity of teachers to work with disadvantaged students.
1.3 Audit objective and scope
The audit objective was to assess the accessibility of mainstream services for Aboriginal Victorians.
The following criteria address the audit objective:
- departments have a sound understanding of the service needs of Aboriginal people
- departments develop and implement effective plans, programs and strategies to facilitate access to services for Aboriginal Victorians and address identified needs
- departments can demonstrate how improved service access has contributed, and is expected to contribute, to improved outcomes for Aboriginal Victorians
- there are effective monitoring, reporting and evaluation frameworks in place, underpinned by reliable data on service access,to demonstrate the achievement of intended outcomes.
This audit examined access to mainstream services for Aboriginal Victorians, including targeted programs and strategies designed to support access to these services, which are mainly services provided or funded by departments.
The audit focused on whole-of-government and departmental policies, programs and strategies, as well as outcomes, covering early childhood, health and human services.
The following departments were part of the audit:
- Department of Premier and Cabinet — Office of Aboriginal Affairs Victoria
- DEECD
- Department of Health
- Department of Human Services.
The audit examined specific services within early childhood, health, and human services — excluding child protection and youth justice. Appendix B sets out the mainstream services and key related strategies and programs provided by departments in this audit.
1.4 Audit method and cost
The audit was conducted in accordance with section 15 of the Audit Act 1994 and Australian Auditing and Assurance Standards. Audit evidence was gathered through:
- meetings with each of the four audited departments, including regional staff
- meetings with service providers and other stakeholders, including in regional areas
- review of government frameworks and policy for Aboriginal affairs
- review of departmental plans, programs and strategies, including examination of evaluations, reviews and progress reports.
Pursuant to section 20(3) of the Audit Act 1994, unless otherwise indicated, any persons named in this report are not the subject of adverse comment or opinion.
The cost of this audit was $335 000.
1.5 Structure of the report
The report is structured as follows:
- Part 2 discusses whether departments have a sound understanding of the needs of Aboriginal Victorians
- Part 3 discusses departmental plans, programs and strategies
- Part 4 discusses access, outcomes and governance.
2 Understanding the needs of Aboriginal Victorians
At a glance
Background
Victorian Government departments need a sound understanding of the service needs of Aboriginal Victorians to be able to design and deliver services which are accessible.
Conclusion
Audited agencies have a reasonable understanding of the service needs of Aboriginal Victorians. However, this is constrained by a lack of broad consultation and complete and reliable data.
Findings
- Audited departments have established both structured and informal processes for consulting and engaging with stakeholders and representatives of Aboriginal organisations. However, existing processes are limited in breadth.
- There are challenges for the audited departments in obtaining complete and reliable data to identify needs, to develop plans, and to evaluate programs and report outcomes, particularly data relating to population levels.
- While there is evidence of data sharing across departments, this is limited and — without improving data collection methods and information-sharing practices — departments cannot be assured they are meeting the needs of Aboriginal people.
Recommendation
That departments improve data collection and recording processes, including collaborating with other departments, Aboriginal community controlled organisations and other relevant organisations to estimate Aboriginal populations for each service.
2.1 Introduction
Departments need a sound understanding of the service needs of Aboriginal Victorians if they are to design and deliver services that are accessible and achieve improved outcomes. This Part assesses whether departments have a sound understanding of the needs of Aboriginal Victorians that can inform the development of robust plans for service delivery.
2.2 Conclusion
Audited departments have a reasonable understanding of the service needs of Aboriginal Victorians. However, this is constrained by a lack of broad consultation and of complete and reliable data. Although there are challenges for the departments in obtaining data to identify needs — including data on population levels — data collection could be improved.
The Department of Health (DH) has an extensive program of evaluation that assists it to understand Aboriginal service needs, but neither the Department of Education and Early Childhood Development (DEECD) nor the Department of Human Services (DHS) were able to demonstrate similarly comprehensive evaluation programs to assist them in understanding the needs of Aboriginal Victorians. DHS and DEECD provided limited evidence of extensive consultation. DH provided evidence of extensive consultation at a state and local level with both mainstream and Aboriginal organisations. However, existing processes are limited in breadth. With respect to consultation:
- Some regional stakeholders indicated that a lack of broad consultation limits community representation and is time-consuming for stakeholders on multiple committees.
- Many organisations, including Aboriginal community controlled organisations (ACCO) that provide feedback and advice to departments are directly funded by those departments, which may diminish their capacity to provide open and constructive feedback. Greater use of community consultation, including with service users, would strengthen the consultation process and provide departments with views unencumbered by funding relationships.
2.3 Understanding Aboriginal service needs
2.3.1 Consultation and engagement
Under the Victorian Aboriginal Affairs Framework (VAAF), consultation and engagement with Aboriginal people is fundamental to the achievement of government objectives for Closing the Gap, and can only be achieved through 'genuine engagement' with both the community and Aboriginal organisations and peak bodies. Under the National Indigenous Reform Agreement (NIRA) to close the gap, Victoria committed to specific service delivery principles for programs and services for Indigenous Australians, including the Indigenous engagement principle:
'Engagement with Indigenous men, women and children, and communities should be central to the design and delivery of programs and services.'
Both VAAF and NIRA make clear the importance of engaging community members as well as ACCOs and mainstream service providers in all aspects of service delivery.
Consultation and engagement is therefore vital to ensure that services are accessible, ensure that planned actions take into account the views and experience of Aboriginal people and the community, and evaluate service effectiveness. There are a number of ways in which government departments consult and engage with Aboriginal organisations and people. These are discussed in this section.

Photograph courtesy of Tobias Titz.
Department of Education and Early Childhood Development
The main consultation process DEECD uses to inform its approach to Aboriginal inclusion involves quarterly meetings with the peak Aboriginal education body in Victoria — the Victorian Aboriginal Education Association Incorporated (VAEAI). DEECD provides funding to VAEAI, which has a committee of management that is made up of the leaders of 32 Local Aboriginal Education Consultative Groups located across the state. Records of meetings are not comprehensive but indicate that these meetings are not used solely for consultation but also to update VAEAI members on DEECD initiatives.
DEECD has a service agreement with the Victorian Aboriginal Community Services Association Limited, with which it has quarterly meetings. DEECD also provided evidence of consultation with the Victorian Aboriginal Child Care Agency and the Victorian Aboriginal Community Controlled Health Organisation.
Evidence provided by DEECD relating to these relationships does not indicate that consultation is robust, nor is it clear if DEECD uses this consultation to assist it in understanding the needs of Aboriginal people. Also, there is insufficient evidence of rigorous engagement with the local community.
However, DEECD does have a reasonable understanding of the needs of Aboriginal people. It has been aware of problems with access to services for some time, evidenced by issues raised in past reports including the State of Victoria's Children 2012: Early Childhood Report which discusses gaps in development between Aboriginal children and the rest of the population.
A departmental review of the maternal and child health (MCH) service in 2013 raised a number of issues with this service, including a lack of strategies to increase the participation of Aboriginal children and families. DEECD has known of issues with the delivery of this service since a 2006 review undertaken when MCH was part of DHS. The recommendations of these reviews are quite similar. For example, both reviews recommended:
- use of outcome, rather than input, measures to monitor and evaluate system performance
- improvements to workforce management models and development of strategies to support the future service delivery model
- implementing a formal professional development program that supports the workforce strategy.
The review findings indicate there has been little change over time in ensuring the MCH service is able to support vulnerable cohorts such as Aboriginal families on a statewide basis. This highlights prolonged inaction by the department in addressing needs and developing and finalising plans and strategies.
Department of Health
DH has a better understanding of the needs of Aboriginal people, obtained primarily through a network of Regional Aboriginal Health Committees that are made up mainly of Aboriginal organisations and local mainstream service providers. DH has developed a range of programs and initiatives, some going back several decades, that aim to specifically address the needs of Aboriginal Victorians — such as the Victorian Patient Transport Assistance Scheme, Koori Maternity Services (KMS) and programs that assist staff with developing culturally safe environments, including Improving Care for Aboriginal and Torres Strait Islander Patients and Aboriginal Hospital Liaison Officers.
A key initiative of DH is the Koolin Balit: Victorian Government strategic directions for Aboriginal health 2012–2022 policy document, which provides the overall strategic directions for Aboriginal health over 10 years.
DH has several ongoing consultation structures in place, including the Victorian Advisory Council on Koorie Health, the Victorian Committee for Aboriginal Aged Care and Disability, and the Aboriginal Tobacco Control Advisory Group. DH provided evidence that the Koolin Balit planning process began with consultation with Aboriginal community-controlled organisations and mainstream community organisations in each region, using both existing consultation structures and a more targeted approach.

Gippsland Lakes Community Health Centre. Photograph courtesy of Tobias Titz.
DH has conducted a number of service delivery reviews, some of which provided valuable information to assist it in understanding Aboriginal needs. These include:
- The Review of KMS 2012 found that barriers to maternity care access include lack of transport, shame, lack of understanding of the importance of maternal health, complex needs, concerns about child protection officers and not trusting the KMS worker.
- The Improving Care for Aboriginal and Torres Strait Islander Patients (ICAP) Quality of Care Review 2011 found that health practitioners need skills and knowledge development to provide care that meets the cultural needs of Aboriginal people.
- The ICAP and Koori Mental Health Liaison Officers Developmental Review 2011 identified key enablers that could improve models of care by meeting the needs of Aboriginal patients.
- The Aboriginal Health Promotion and Chronic Care Program (AHPACC) Review 2010 found that the program may have contributed to a 69 per cent increase in access to medical services between 2005–06 and 2009–10.
- DH used the results of these and other reviews when developing Koolin Balit, including the shift in focus away from shorter 'one-off' projects to more long-term work. DH also changed the structure of its ICAP program following the ICAP and Koori Mental Health Liaison Officer (KMHLO) Developmental Review in 2011 and used the 2010 evaluation of the AHPACC program to revise service delivery targets and models, improve networking and shift resourcing to capacity-building activities.
These reviews improved DH's understanding of the needs of Aboriginal people. In particular, DH applied the results of its ICAP and KMHLO Developmental Review to redesign the program, and recently completed a series of evaluations of its previous overarching Aboriginal health strategy, the Closing the Gap in Aboriginal Health Outcomes Initiative, which also recommended a shift away from one-off projects to more sustained initiatives.
Department of Human Services
In December 2012, DHS restructured its operations hierarchy to increase its focus on service needs at the local level. The aim of this was to improve service coordination and provide better outcomes through early intervention and increasing social and economic participation. Human Services stakeholders indicated the importance of understanding localised differences in needs. The restructure may assist in developing a better understanding of this.
DHS has processes in place for structured consultation and informal engagement with stakeholders and representatives of Aboriginal groups. These include the Community Conversations and Human Services Aboriginal Roundtable, and engagement processes with six Aboriginal Signatory Organisations. Formal meetings are held at scheduled times throughout the year. In March 2013, the chief executive officers of these organisations and the Secretary of DHS signed the DHS protocol, which formalises the engagement process.
Despite these formal processes, evidence does not indicate that consultation is rigorous and it is unclear how it is used to inform an understanding of needs. However, DHS is in the process of implementing broader consultation processes. These include Community Conversations held in conjunction with the Human Services Aboriginal Roundtable, and DHS's relationship with the First Peoples Disability Network Australia and the Victorian Aboriginal Disability Network, which represent Aboriginal people with a disability and their carers.
DHS advised that its four divisions are working with local communities to establish Aboriginal advisory structures to support planning and implementation of Aboriginal inclusion action plans. These consultation processes are recent initiatives, so it is too early to assess their effectiveness.
DHS has undertaken program reviews and developed guidance material and discussion papers in relation to its disability, housing and homelessness services. Our review of these documents highlighted challenges for the department in understanding and addressing the service needs of Aboriginal Victorians in these areas.
Aboriginal Homelessness in Victoria
A discussion paper on Aboriginal homelessness prepared by DHS in 2013 indicated that based on Australian Bureau of Statistics (ABS) data the number of Aboriginal people experiencing homelessness had increased by 30 per cent between 2006 and 2011 — from 639 people to 832 people. The number of all homeless people in Victoria also increased by 30 per cent over the same period.
The paper identified the structural barriers to access experienced by Aboriginal Victorians, including financial pressures and lack of culturally responsive services, and weaknesses in the reliability of data on homelessness. The paper recommended that:
- agencies should build the evidence-base for Aboriginal homelessness and separate out data to capture Aboriginal service usage to inform future distribution of funding addressing community needs and disadvantage
- Aboriginal people should be engaged in the development, implementation, monitoring and evaluation of policies and programs.
This paper provides an informative insight into how DHS can identify and understand the housing needs of Aboriginal Victorians and address homelessness issues.
Aboriginal Victorians with a disability
In March 2011, DHS released a guide for promoting access and inclusion of Aboriginal Victorians with a disability entitled Enabling choice for Aboriginal people living with a disability.
The guide acknowledged that the disability needs of Aboriginal Victorians are complex and may require access to a range of services and supports, as well as increased coordination between services. It also identified that the factors contributing to Aboriginal use, or non-use, of disability support services are complex, ranging across fear, racism, stereotyping, misinformation, shame, attitudes towards Aboriginal clients among service providers, and the interpretation of how disability is defined within the Aboriginal community.
This guidance material was based on consultation with ACCOs, community elders and local community disability service providers. It provides evidence of DHS's efforts to understand the needs of Aboriginal Victorians with a disability and the provision of disability services.
2.3.2 Complete and reliable data
Complete and reliable data is important to:
- assist with the identification of Aboriginal service needs, leading to the planning and development of evidence-based departmental programs
- measure the success of a program, including whether service access has improved, and expected outcomes have been achieved.
There are challenges for the audited departments in obtaining complete and reliable data to identify needs, to develop plans and to evaluate programs and report outcomes — particularly data relating to population levels. For example, ABS cannot calculate and report Aboriginal life expectancy in Victoria, because the number of deaths reported as Aboriginal is too low and the population is too small. This means that data about a key outcome is not presently available, and it is not expected to be until after the 2016 census.
Some programs that encourage identification, such as those used in public hospitals, assist in developing a better understanding of population levels in local areas. However, in order to understand the service needs of the Aboriginal population, departments should further develop strategies to increase identification, and work with local service providers and ACCOs to assist in understanding population levels in local areas. This is particularly pertinent when estimating Aboriginal service use in regional areas. For example, 2006 ABS data put the Aboriginal population in the Shepparton area at 3.2 per cent of the overall population. Based on its number of registered clients, Rumbalara Aboriginal Cooperative estimates the population to be 7.4 per cent. Greater Shepparton City Council has estimated that the population may be as high as 10 per cent.
Departments are aware of barriers to access. However, high annual population growth rates, particularly in regional areas, mean it is difficult for departments relying on census data to be confident that all of the eligible people who require a service are able to access it. This is why estimated service populations — that is, a population estimate based on demand for and use of services in a particular area — can be more useful.
Both DH and DHS have put in place data collection initiatives to improve completeness and reliability of datasets, particularly relating to service accessibility for Aboriginal Victorians. For example, DH is establishing more accurate baseline data on Aboriginal populations in hospitals, while DHS has established the Centre for Human Services Research and Evaluation, which is focusing on developing its evidence-base. DEECD is in the process of improving data collection in the MCH service.
While there is evidence of data sharing across departments, this is limited, and without improving data collection methods and information-sharing practices, departments cannot be assured they are meeting the needs of Aboriginal people.
Department of Education and Early Childhood Development
Past reports at DEECD have highlighted data quality issues affecting the evaluation of service delivery programs. For example, the 2006 MCH service review — undertaken by DHS — found that data quality issues make evidence-based research, and consequently measuring outcomes, difficult. The September 2013 VAGO report Performance Reporting Systems in Education found similar problems with data quality. This report noted it is difficult to monitor who is not using the MCH service or the reasons why this is occurring.
These reports indicate that DEECD has for a number of years known about data quality issues affecting evaluation of access to services. DEECD provided evidence that it is in the process of establishing a central data system for the MCH service to replace manual data collection processes in response to VAGO's findings.
Department of Health
DH does not set service access targets for Aboriginal people as part of its approach to ensuring mainstream services are accessible. While this makes it difficult for DH to determine if mainstream services are becoming more accessible, problems with data mean that it would be difficult to measure access without considerable work to quantify the Aboriginal population.
Since 1993, mandatory identification of Aboriginal people in the Victorian Admitted Episodes Dataset has enabled the establishment of baseline data. DH is endeavouring to establish more accurate baseline data by encouraging identification of Aboriginal users of DH services — including hospital and dental, home and community care, Victorian eye care and community health services, and as part of AHPACC. This initiative is significant because it provides DH with data on actual service use, which is more useful than relying on ABS census data which estimates the temporary population of a particular area.
The ICAP program supports identification of Aboriginal patients in hospitals by aiming to create a more welcoming environment. Evidence indicates that ICAP has:
- improved cultural safety and support in public hospitals
- increased numbers of referrals
- decreased fail-to-attend rates at hospitals.
The establishment of baseline data and the ICAP program are both positive initiatives for DH.
Department of Human Services
DHS provided data relating to Aboriginal people for specific service areas including detailed data relating to provision of public housing, overcrowding and total numbers of new households assisted. DHS estimated the proportion of the Aboriginal population in Victoria that was homeless in 2013 to be 3.7 per cent. However, the reliability of this data is unclear. DHS advised that it is working to improve data reliability, particularly regarding accessibility of services for Aboriginal people.
DHS also advised that it has completed work to incorporate specific service data relating to Aboriginal Victorians into DHS board and other performance reporting, including housing assistance waiting times, access and eviction data. DHS also informed us that work is underway to address the reliability of service data for disability and homelessness services. For example:
- DHS is developing a Client Engagement Framework — consistent with the Victorian Government Aboriginal Inclusion framework — to improve client engagement across settings and promote culturally responsive service delivery, including a Practice Guide to support the identification of Aboriginal clients.
- Work is being undertaken to forecast service demand for homelessness services as part of the Victorian Homelessness Action Plan 2011–15, which includes a specific focus on Indigenous clients.
We have not seen evidence of this work.
DHS has established the Centre for Human Services Research and Evaluation, which will lead the development of DHS's evidence-base through research and evaluation activities, and advise and assist DHS in evaluating program areas.
Recommendation
- That departments improve data collection and recording processes, including collaborating with other departments, Aboriginal community controlled organisations and other relevant organisations to estimate Aboriginal populations for each service.
3 Plans, programs and strategies
At a glance
Background
Plans, programs and strategies should be consistent with the Victorian Aboriginal Affairs Framework (VAAF) and demonstrate how each department will improve access and inclusion for Aboriginal people across all service areas.
Conclusion
Plans, programs and strategies do not yet adequately reflect the service access criteria of the VAAF.
Findings
- All departmental secretaries have agreed to finalise Aboriginal inclusion action plans by the end of August 2014, but significant work remains to ensure that plans identify and address barriers to access.
- There is a lack of collaboration and coordination between the departments and service providers, as well as at service delivery level between local providers.
- While the Office of Aboriginal Affairs Victoria has released guidelines to develop Aboriginal inclusion action plans, departments are responsible for developing and implementing their own plans. There is little oversight of plans which means they are of varying quality.
Recommendations
That departments:
- as a priority, finalise Aboriginal inclusion action plans and fully apply VAAF service access criteria in service delivery plans and programs
- engage a broad range of Aboriginal people in developing, implementing, monitoring and evaluating plans and programs
- identify and pursue opportunities to collaborate, cooperate and share data with government agencies responsible for mainstream service delivery and with service providers.
3.1 Introduction
Plans, programs and strategies should be consistent with the Victorian Aboriginal Affairs Framework (VAAF) and demonstrate how each department will improve access and inclusion for Aboriginal people across all service areas.
The Victorian Government Aboriginal Inclusion Framework 2011 (VGAIF) requires all government departments to prepare Aboriginal inclusion action plans in accordance with the Aboriginal Inclusion Action Plan Guidelines issued by the Office of Aboriginal Affairs Victoria (OAAV) in 2011. Under VGAIF, these plans must demonstrate how each department will improve access and inclusion for Aboriginal people across all service areas.
VGAIF is flexible about the form these plans may take and plans do not consistently demonstrate how inclusion and access will be improved.
Departments are responsible for developing, releasing and implementing their own plans. The framework is intended to allow departments to tailor their plans and programs to suit their particular role and approach to facilitating access and delivering the services they provide or fund.
This Part assesses audited departments' plans, strategies and programs for enhancing access to and delivery of mainstream services for Aboriginal Victorians.
3.2 Conclusion
Departments have developed a range of plans, strategies and programs to assist in improving access. Most of these have been in place for five to 10 years, and in the case of the Department of Health (DH), some for over 20 years. However, despite the development of VAAF in 2012, departments have neither reviewed, nor updated, nor significantly changed their plans to reflect VAAF's shift in focus to improving service access. Plans were due to be finalised by the end of 2013 but were not completed by that date. All departmental secretaries have now agreed to finalise outstanding Aboriginal inclusion action plans by the end of August 2014.
There is little oversight of plans which means they are of varying quality. OAAV advised that the Secretaries' Leadership Group on Aboriginal Affairs (SLG) has recently agreed to a terms of reference for the creation of a new interdepartmental Aboriginal inclusion working group to provide for regular departmental engagement and oversight of the plans and associated processes.
While departments have addressed some access barriers through their plans, programs and strategies, barriers have not been uniformly addressed and it will be difficult to achieve better outcomes without considering all the issues that impact service access.
3.3 Adequacy of plans and strategies for service delivery
We examined the progress of audited departments in preparing Aboriginal inclusion action plans under the VGAIF and VAAF, as well as past Aboriginal service delivery plans and strategies to assess whether they were consistent with better practice criteria established in government policy framework documents.
3.3.1 Quality of plans and strategies
The quality of the sample of plans and strategies for delivery of services to Aboriginal Victorians was poor overall and did not adequately address many of the better practice criteria. There is significant scope for departments to improve the comprehensiveness of these documents.
Aboriginal inclusion action plans should have clearly stated objectives, expected outcomes with clear targets, performance measures that are capable of being measured and time lines. Plans will need to incorporate accountabilities through roles and responsibilities, provide for effective monitoring and evaluation, and have clear lines of reporting, including internally, to OAAV and the SLG, and through the annual report.
3.3.2 Department of Education and Early Childhood Development
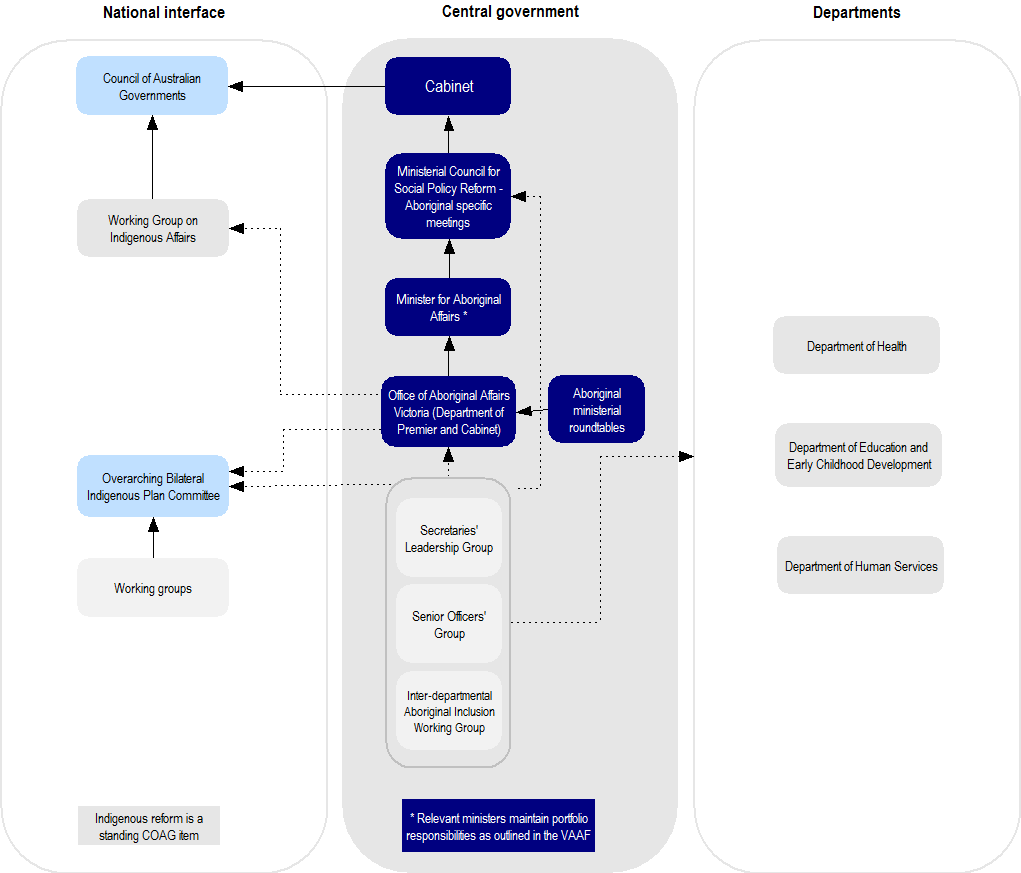
We assessed two of the Department of Education and Early Childhood Development's (DEECD) key strategic documents for the provision of Aboriginal education services against government policy framework objectives and better practice criteria. Figure 3A summarises the results of our assessment.
Figure 3A
DEECD–Assessment of plans and strategies against key criteria
Note: ✔ = Met, P = Partially met and ✘ = Not met.
Source: Victorian Auditor-General's Office based on government policy framework documents.
Wirnalung Ganai — Aboriginal Inclusion Action Plan
DEECD has a whole-of-department action inclusion plan, Wirnalung Ganai: Our People–Aboriginal Inclusion Action Plan 2012–14, which was launched in 2011. It aims to make DEECD a more culturally responsive workplace, both structurally and organisationally, and to increase its employment of Aboriginal people in order to facilitate a more culturally appropriate approach to departmental service delivery.
Overall, this plan does not meet better practice criteria for a soundly based action plan. It does not reflect VAAF access criteria, detailing only that access will be improved by increasing Aboriginal employment and making the workplace more culturally safe.

Photograph courtesy of Tobias Titz.
Garrin Garrin — A strategy to improve learning and development outcomes for Aboriginal Victorians (draft)
DEECD is currently developing an Aboriginal education strategy, which when released will replace its previous Aboriginal education strategies, Wannik and Wurreker, and become DEECD's main strategy for Aboriginal inclusion.
This draft strategy revises the early years approach into a lifespan approach to Aboriginal education, and it aims to 'improve the opportunities for all learners without exception'. The draft strategy indicates that 'being available and being accessible are two different things', emphasising the difficulties Aboriginal people may face in accessing services, and highlighting the need for the department to continue to work to improve service access, inclusiveness and usefulness.
Although barriers are mentioned, they are not explicitly identified. DEECD consulted with community members across Victoria as part of the development of the strategy.
Specifically, the draft strategy discusses the difference between a service being available and it being accessible, and references VAAF accessibility criteria. However, there are no clear target measures or milestones mentioned outside of those under VAAF.
3.3.3 Department of Health
DH has a range of strategic documents and plans for enabling Aboriginal inclusion, including the Department of Health Aboriginal Inclusion Framework 2013, Koolin Balit: Victorian Government strategic directions for Aboriginal health 2012–2022 and various regional closing the gap plans.

Photograph courtesy of Tobias Titz.
We assessed a number of DH's strategy documents and plans against government policy framework objectives and better practice criteria. Figure 3B summarises the results of our assessment.
Figure 3B
DH–Assessment of plans and strategies against key criteria
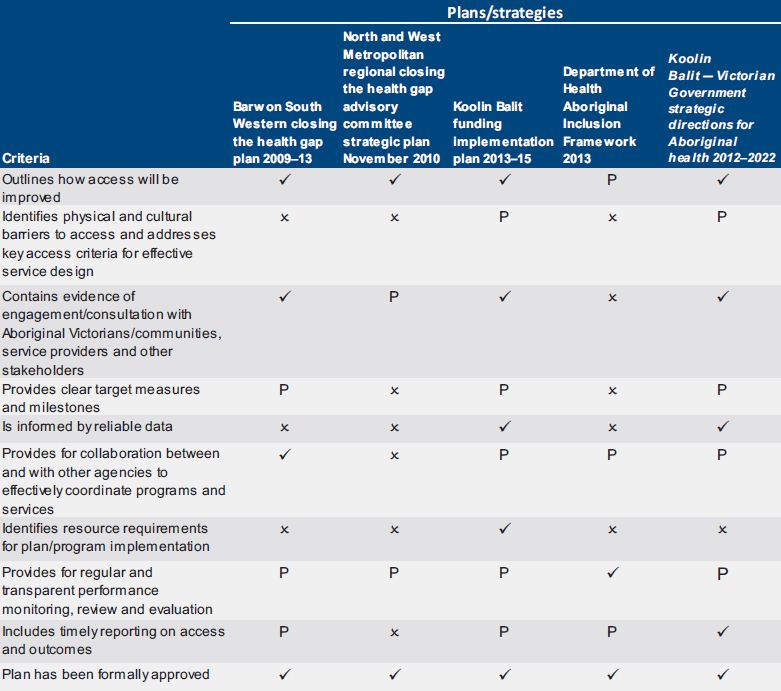
Note: ✔ = Met, P = Partially met and ✘ = Not met.
Source: Victorian Auditor-General's Office based on government policy framework documents.
Regional closing the gap plans
We assessed two regional plans — Barwon South Western closing the health gap plan 2009–13 and North and West Metropolitan regional closing the health gap advisory committee strategic plan November 2010. These plans were developed prior to the introduction of VAAF, and therefore do not reflect VAAF access criteria.
Both plans were formally adopted, and they adequately describe how access will be improved. However, each plan was deficient with respect to other criteria — neither adequately identifies or addresses barriers to access, and they do not include clear target measures and milestones, resource needs or requirements for reporting on access and outcomes.
DH advised that obtaining data at the local level relating to incidence of disease or, for example, perinatal mortality is difficult because of the very small sample sizes. In many cases it is difficult to provide de-identified data.
Plans/strategies under the Victorian Aboriginal Affairs Framework
The DH Aboriginal Inclusion Framework 2013 sets out DH's key strategies and plans to promote access and inclusion. It emphasises local planning as imperative to meeting needs, including the need for targeted intervention for Aboriginal people. Under this framework, DH has developed its plan Koolin Balit — Victorian Government strategic directions for Aboriginal health 2012–2022.
While these documents do not directly reference VAAF, DH believes that VAAF service access criteria are implicit in them, and that Koolin Balit was prepared with frequent interaction between DH and OAAV relating to themes and direction, although it was published six months prior to VAAF. However, VAAF access criteria are quite specific, and without direct reference to these criteria it is difficult to see how they are being applied to service delivery.
DH has recently completed the Koolin Balit funding implementation plan 2013–15, which contains an overarching plan for funding Koolin Balit initiatives, including the Koolin Balit regional action plans. The funding plan is linked to VAAF and Koolin Balit: Victorian Government strategic directions for Aboriginal health 2012–2022. We have been given extensive documentation indicating significant consultation and planning has been undertaken in regional areas relating to the development of this framework and the individual regional plans.
As well as these plans, individual hospitals and health services have adapted and developed a number of their own initiatives to improve access to services. These include local advisory committees, and cultural awareness training that is targeted to specific local cultural needs, as is the case at Goulburn Valley Health, which has a memorandum of understanding (MOU) with the Rumbalara Aboriginal Cooperative. Feedback from Aboriginal stakeholders indicated that this has been a positive approach.
Mallee District Aboriginal Services has developed a number of MOUs, including with Mildura Base Hospital. These MOUs provide an opportunity for mainstream organisations to strengthen their cultural awareness and relationships with the local community, and are viewed as a positive development by both organisations.
3.3.4 Department of Human Services
Since around 2002, the Department of Human Services (DHS) has developed a range of action strategies and plans to enable Aboriginal inclusion. These have evolved over time — with the introduction of the Victorian Indigenous Affairs Framework in 2006, the Aboriginal Inclusion Framework in 2011 and more recently VAAF in 2012.
Prior to the restructure of DHS in 2012, in addition to overarching departmental action plans for Aboriginal services delivery, the former eight departmental regions were required to develop individual Aboriginal services plans. The four newly created divisions are required to develop Aboriginal inclusion action plans that are consistent with VAAF principles and criteria.
We assessed a number of the department's strategic documents and plans against government policy framework objectives and better practice criteria. Figure 3C summarises the results of our assessment.
Figure 3C
DHS–Assessment of plans and strategies against key criteria
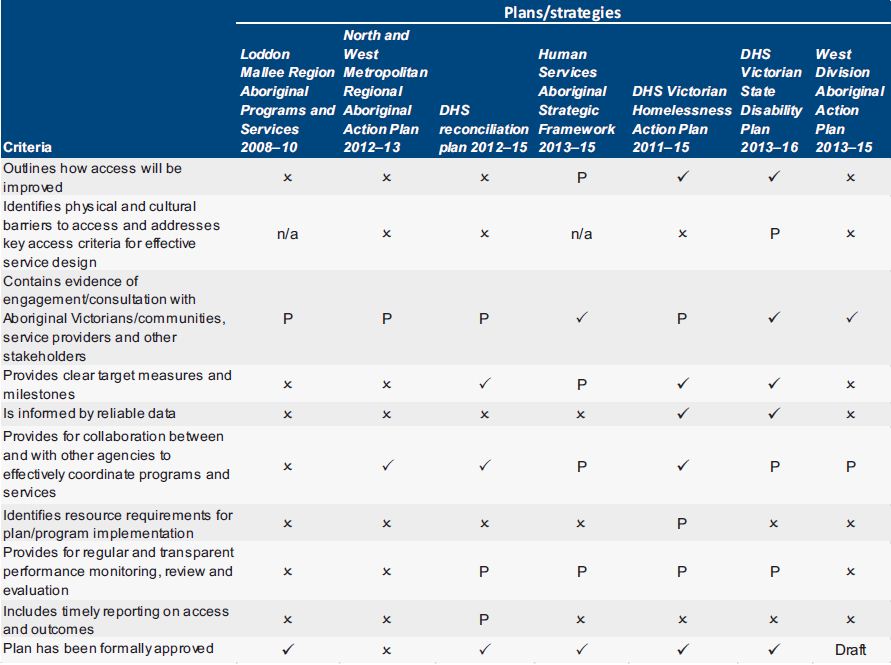
Note: ✔ = Met, P = Partially met, ✘ = Not met and n/a = Not applicable.
Source: Victorian Auditor-General's Office based on government policy framework documents.
Regional service delivery plans
We reviewed plans prepared by two of the former DHS regions — Loddon Mallee Region Aboriginal Programs and Services 2008–10 and the North and West Metropolitan Region Aboriginal Action Plan 2012–13. Neither plan fully satisfied any of the criteria for a robust plan. Further, a number of these regional plans developed over the past 10 or so years had not been reviewed or updated. The department was unable to provide any plan for the former Grampians Region.
Plans/strategies under VAAF
Human Services Aboriginal Strategic Framework 2013–15
In response to the VGAIF and VAAF, DHS developed the Human Services Aboriginal Strategic Framework 2013–15. This framework establishes six priority areas and includes nine stated objectives for Aboriginal inclusion, one of which is to 'increase access and quality of services to Aboriginal clients across the service system, including mainstream and departmental services'.
The DHS framework clearly links with VAAF and its objectives and will be useful in guiding the development of DHS's Aboriginal inclusion action statement and the divisional plans.
The DHS framework provides 59 key deliverables under the priority areas, including that the department will develop the DHS Aboriginal inclusion action statement. In the framework document these deliverables and associated performance indicators consist of broad, general statements, and it is unclear how DHS intends to accurately measure them.
Photograph courtesy of Tobias Titz.
Divisional Aboriginal action plans
The department's four divisions are required to develop Aboriginal action plans consistent with the Human Services Strategic Framework 2013–15. DHS is also developing an Aboriginal inclusion action plan/statement to accord with the VGAIF. The plan/statement is expected to be completed by August 2014.
We examined the DHS draft plan for West Division. While we acknowledge this is an early draft, it is not comprehensive, consisting of only two pages of general statements on actions and expected outcomes. DHS advised that final plans for all four divisions will include objectives, accountabilities, time lines and monitoring and progress measurement.
Divisional plans are being developed in consultation with Aboriginal communities. These documents are drafts as they are still to be endorsed by local advisory groups.
Department of Human Service Standards
Good practice noted in DHS is the development of the Human Service Standards in July 2012. These standards represent a single set of service quality standards for department-funded service providers and department-managed services. The Standards promote client empowerment, access and engagement, wellbeing and participation.
DHS intends to review service provider compliance to the Standards every three years.
3.4 Collaboration and coordination
There is a lack of effective collaboration and coordination at all levels, both between departments, between departments and service providers, and at service delivery level between local providers.This is evident from our discussions with Aboriginal stakeholders and our examination of departmental reviews and evaluations.
Feedback from Aboriginal stakeholders and service providers was that the problem with government services is the 'siloed' approach to service delivery, which can impede access and impact outcomes. This creates difficulties for users, who have to navigate multiple service providers to access services.
In 2012, the former Department of Planning and Community Development commissioned a review to provide advice on a measurement and evaluation framework for monitoring and evaluating access by Aboriginal people to mainstream services, which OAAV used in developing aspects of VAAF. This report highlighted a need for greater collaboration and cooperation between entities that are delivering services.
A 2006 maternal and child health (MCH) service evaluation undertaken when the service was run by DHS also noted that new strategies and adaptations in service delivery were driven by local initiatives, rather than at a statewide level. Similarly, the 2013 MCH service review indicated that the MCH service should adopt localised examples of innovation and collaboration.
A lack of effective collaboration across departments and service providers impedes access to a service as illustrated in the case study in Figure 3D.
Figure 3D
Availability of transport to kindergarten
|
For some Aboriginal families transport to kindergarten is crucial for kindergarten services to be accessible. Aboriginal children are eligible for free kindergarten, but the usefulness of this program is diminished if other criteria, such as convenience and accessibility, are not addressed. While DEECD funds schools to coordinate the school bus program and Public Transport Victoria (PTV) funds the cost of running the buses, such funding is not provided for transport to kindergarten, although there is evidence that some children in regional locations cannot access kindergarten without transportation. DEECD advised that it is not responsible for kindergarten transport, which demonstrates the need for coordination across agencies. In order for kindergarten programs to meet VAAF access criteria, collaboration with relevant agencies such as PTV is required. If this does not happen, barriers to access to kindergarten will persist. |
Source: Victorian Auditor-General's Office.
We noted a positive initiative is the development of Victoria's Vulnerable Children Our Shared Responsibility Strategy 2013–2022 released in May 2013, administered by DHS. The strategy is a partnership involving DEECD, DH, DHS and Victoria Police. It proposes to build 'local networks' to ensure local information sharing, and coordination of service provision and planning to improve outcomes for vulnerable children and families.
Recommendations
That departments:
- as a priority, finalise Aboriginal inclusion action plans and fully apply Victorian Aboriginal Affairs Framework service access criteria in service delivery plans and programs
- engage a broad range of Aboriginal people in developing, implementing, monitoring and evaluating plans and programs
- identify and pursue opportunities to collaborate, cooperate and share data with government agencies responsible for mainstream service delivery, and with service providers.
4 Access, outcomes, monitoring and reporting
At a glance
Background
The Victorian Aboriginal Affairs Framework (VAAF) states that increased access to services will lead to improved outcomes for Aboriginal Victorians. Departments need to undertake robust planning, monitoring and reporting to identify and address barriers to access.
Conclusion
Access to services has increased in some instances, which is encouraging, but there has been little improvement in outcomes — and in some cases the gap has widened. The Office of Aboriginal Affairs Victoria and the Secretaries' Leadership Group on Aboriginal Affairs (SLG) could better monitor and coordinate the implementation of VAAF.
Findings
- With the exception of the Department of Health, there is little evidence of comprehensive evaluations that assess the achievement of outcomes for Aboriginal Victorians.
- Weaknesses in data make it difficult for departments to accurately measure the achievement of outcomes and effectively monitor, evaluate and report progress on service delivery plans.
- Reporting is not comprehensive and does not provide a clear understanding of whether access is improving or outcomes are being achieved.
Recommendations
That departments:
- routinely evaluate plans and programs to determine whether access is increasing and outcomes are improving, and to identify where improvements are needed
- develop internal and external reporting regimes on progress and outcomes.
That the Department of Premier and Cabinet:
- provides more active leadership and direction to make sure that departmental programs and strategies comply with VAAF
- through the SLG, monitors the implementation of departmental plans, evaluates outcomes and monitors the development of investment logic maps that identify funding requirements over the term of the government's commitment to VAAF.
4.1 Introduction
The achievement of specific targets and outcomes is a key aspect of the Victorian Aboriginal Affairs Framework 2013–18 (VAAF). Without effective monitoring, evaluation and reporting, agencies cannot determine whether they have achieved or are achieving, their strategic goals. VAAF states that 'improved access will lead to improved outcomes for Aboriginal Victorians'.
Research indicates that access to services, such as early childhood, health and housing services, can lead to more positive outcomes at both the community and individual level. Aboriginal people have poorer outcomes across a range of indicators of health and wellbeing. VAAF aims to address this disparity by 'improving the life expectancy, wellbeing, economic prosperity and quality of life of Aboriginal Victorians'.
This Part examines departments' progress in measuring access and achieving outcomes for Aboriginal Victorians.
4.2 Conclusion
There is significant scope for the departments to improve their current arrangements for monitoring, evaluating and reporting on outcomes of Aboriginal service delivery strategies and programs. Departments measure access in many of their programs and services. However, with the exception of the Department of Health (DH), they do not conduct comprehensive evaluations that assess the achievement of outcomes for Aboriginal Victorians and cannot demonstrate improvements in service access as a result of many of their programs.
This means departments cannot understand whether their plans, programs and strategies are improving access to services and achieving positive outcomes to close the gap in line with state and Commonwealth targets.
The Office of Aboriginal Affairs Victoria (OAAV) does not monitor outcomes, and the lack of oversight and coordination means that VAAF is not being implemented effectively.
4.3 Access to services
4.3.1 Measuring access
A focus on access is imperative for improving outcomes for Aboriginal Victorians. Access to services is a key aspect of the VAAF approach to closing the gap. Departments cannot be assured that access to services is improving and better outcomes are being or will be achieved without suitable mechanisms to measure accessibility.
Improvements to accessibility were found at DH, the Department of Human Services (DHS) and the Department of Education and Early Childhood Development (DEECD). At DH this improvement has been across a range of areas, while at DEECD, gaps in participation in maternal and child health (MCH) services and kindergarten have narrowed. DHS can demonstrate improvements in access to public housing and homelessness services.
Department of Health
Through evaluations of Aboriginal Quitline, Aboriginal Health Promotion and Chronic Care Program (AHPACC), and Improving Care for Aboriginal Patients (ICAP), DH can demonstrate that access has improved for Aboriginal Victorians in a number of its mainstream services:
- Quitline
- Community Health
- Hospitals.
In particular, ICAP has assisted in the establishment of baseline datasets in hospitals that can be used to inform program design and estimate service user populations, which is a positive step in measuring access to services. In 1993, DH established mandatory identification of Aboriginal people through the Victorian Admitted Episodes Dataset, enabling a baseline for measuring access in data on Aboriginal inpatient hospital admissions.
DH also uses the Program Report for Integrated Service Monitoring, which monitors Aboriginal admissions and presentations at every health service and public hospital. ICAP encourages the creation of a more welcoming environment in hospitals — for example, through flexibility in visiting rules and culturally appropriate work practices — which means increases in access of hospital services and willingness of Aboriginal patients to self-identify can be attributed in part to this program.

Photograph courtesy of Tobias Titz.
Department of Education and Early Childhood Development
DEECD measures access to kindergarten services and the MCH service, although there are problems with the completeness and reliability of the data, which is entered manually and — in the case of three-year-old kindergarten, is measured against Australian Bureau of Statistics (ABS) population projections, which are not a reliable estimate of the service user population. However, DEECD is working to improve data systems in the MCH service. DEECD measures participation in four-year-old kindergarten against Aboriginal enrolments in prep the following year, which it suggests gives a more accurate picture than relying on ABS projections.
Although DEECD meets the National Minimum Standard by taking attendance in August Census Week, the absence of attendance rates across the year in kindergarten limits comprehensive measurement of service accessibility.
Department of Human Services
DHS measures access to public housing and homelessness services for Aboriginal Victorians. It has undertaken work to understand why disability services may not be accessed and what can be done to improve them. Disability Services, Closing the Gap Project assessed local initiatives relating to disability services access. It found that Aboriginal people are not accessing disability services in regional areas and there is a lack of complete and reliable data on Aboriginal Victorians with a disability. DHS should continue to improve its strategies for measuring access so that it can identify issues and use data to improve programs, evaluate achievement of outcomes and track progress toward targets.
4.3.2 Improvements in access
To improve outcomes for Aboriginal Victorians and to close the gap with the rest of the population, increases in access to services are required. The relatively small Aboriginal population in Victoria means that when analysing improvements in service access, it is important to consider long-term trends in access levels, rather than sharp increases or decreases in access over a couple of years.
This is demonstrated by Appendix C, Progress toward targets — which indicates that since 2009, although there have been fluctuations in the perinatal mortality rate, there has been an overall trend downwards since 2004.
Department of Education and Early Childhood Development
At DEECD, there has been steady improvement in participation rates in MCH services. While participation declined between 2011–12 and 2012–13, longer-term trends indicate that it is increasing. Despite the existence of the kindergarten grants program, kindergarten participation did not significantly improve from 2001 to 2011, although there was a sharp increase in participation in 2012. In both these cases, it is best to view medium- or long-term trends, rather than sharp increases or decreases over a couple of years. This means that results are mixed.
DEECD provided the 2013 review of the MCH service, but this did not evaluate the outcomes or impact of attending the service. The review was driven by the need for 'an increased focus' on achieving better outcomes for children, which is a positive step. However, DEECD has not evaluated its kindergarten grants program. While the improvement in kindergarten participation in 2012 is positive, taking into account trends over the past decade, it is not likely that the VAAF target to close the gap in kindergarten participation by 2014 has been achieved. The absence of evaluation means that DEECD is not in a position to understand why this may be the case.
Department of Health
In its 2011 report Access to health services for Aboriginal and Torres Strait Islander people the Australian Institute of Health and Welfare indicates that in Victoria the level of identification of Aboriginal patients in admitted patient data means that the data is of sufficient quality for analysis. Identification in hospitals has steadily increased over time, which means that DH can now see that the rate of Aboriginal people leaving hospital without treatment or against medical advice has decreased, which is a positive development.
DH provides a 30 per cent loading on payments for Aboriginal hospital patients, which enables hospitals to employ Aboriginal Hospital Liaison Officers and other additional supports and system changes as detailed in the ICAP program. The loading also provides an incentive for identification of Aboriginal background which in turn provides a more accurate picture of rates of access to hospitals. The increased willingness to self-identify as Aboriginal in hospital settings is a positive step and may indicate that hospitals have become more welcoming environments over time. DH's evaluation of the Closing the Gap in Aboriginal Health Initiative found that greater focus on culturally responsive practice has positively influenced service delivery outcomes.
However, improvements are mixed. In aged care assessment numbers for Indigenous clients have remained steady since 2007–08. Although the gap has narrowed over a 10-year period, the rate of Aboriginal referrals is lower than would be expected taking into account population levels.
Department of Human Services
At DHS, data is not sufficiently complete or reliable to draw strong conclusions about the extent to which accessibility of services is improving. The Victorian Government Aboriginal Affairs Report 2013 found that in 2012–13, Aboriginal Victorians accessed homelessness services at a rate of 8.9 per cent of all clients, an increase from 8.0 per cent in 2011–12. This indicates an improvement in service accessibility. However, the rate of access may be the result of an increase in the number of Aboriginal people who are homeless, and it is not clear if the rate of access is proportionate to the rate of need within the Aboriginal population.
Within public housing, access has improved from 1 396 households in 2008–09 to 1 784 households in 2012–13. While the increase in rates of residence in public housing is positive, DHS has not provided any evidence that indicates whether increases in access are sufficiently meeting demand for housing.
4.4 Measuring outcomes
Evaluation is required to assess whether programs are providing the kind of short-term benefits that may lead to increased access and long-term positive outcomes for Aboriginal Victorians. Departments should use evaluation to determine whether programs are contributing to outcomes and — where evaluations identify lessons or opportunities for improvements — adjust their strategies, plans, programs or service delivery accordingly. Without effective evaluations, departments cannot be assured they are on track to achieve VAAF targets.
4.4.1 Department of Health
Of the audited departments, only DH demonstrated a comprehensive evaluation program that assesses outcomes and has been in place for a number of years. As well as program level evaluations, DH evaluated its previous Closing the Gap in Aboriginal Health Initiative, including on the basis of increases to access and the achievement of outcomes. DH has recently established an evaluation and evidence working group specifically focused on Aboriginal health.
DH provided the following evaluations:
- Aboriginal Health Promotion and Chronic Care
- Koori Maternity Services
- Victorian Patient Transport Assistance Scheme
- ICAP and Koori Mental Health Liaison Officers developmental review
- interim and final evaluations of the Closing the Gap in Aboriginal Health Initiative.
- The evaluation regime at DH assists it in understanding the effectiveness of its programs. DH has been able to analyse short-term outcomes through its program evaluations, as well as long-term impacts through evaluations of the Closing the Gap in Aboriginal Health Initiative.
4.4.2 Department of Education and Early Childhood Development
DEECD's statewide MCH service, including enhanced care, was reviewed in 2006 and 2013. The 2006 review was conducted by DHS as it had responsibility for the MCH service at that time. These are useful reviews that provide recommendations for improvements. However, the 2013 review commented that the main performance measure used by the MCH service is output based, and recommended that it adopt a program logic and outcomes-based framework.
DEECD also provided an evaluation of its statewide Best Start program, which contained two case studies of Aboriginal Best Start programs, but no reviews or evaluations of its other programs that are specifically designed to assist access for Aboriginal people. Through collaboration between different local services Best Start aims to assist vulnerable sections of the population to receive early childhood services.
DEECD advised that it intends to evaluate the Koori Preschool Assistants program in 2014, and is currently undertaking an evaluation of its In Home Support and Home Based Learning Programs. The Best Start evaluation included reporting on numbers attending kindergarten, breastfeeding rates and attendance at MCH services. This provided useful information to understand whether local Best Start programs are achieving positive results. The MCH reviews conducted in 2006 and 2013 made some similar recommendations, indicating little change in service delivery since 2006.

Photograph courtesy of Tobias Titz.
4.4.3 Department of Human Services
DHS provided evaluations, relating to disability and homelessness services. This included the Opening Doors Framework — relating to homelessness and social housing service provision — Elizabeth Street Common Ground Supportive Housing Project and the Community Prevention Initiative, the latter of which was funded as part of the Victorian Indigenous Family Violence Strategy. While these evaluations analysed outcomes for all Victorians receiving specific services and they considered Aboriginal access — they did not specifically focus on access and outcomes for Aboriginal Victorians.
DHS also provided project reports for the Regional Aboriginal Homelessness Project, which was conducted in the former North West Metro region in 2011. These reports provided useful recommendations for system-wide improvement, and involved consultation with Aboriginal clients. However, overall, the evaluation regime at DHS does not adequately address accessibility of mainstream services for Aboriginal Victorians.
Neither DEECD nor DHS can demonstrate an effective and useful evaluation regime for Aboriginal programs, and it is not clear how these agencies can be assured their plans, programs and strategies are achieving positive outcomes for Aboriginal people.
4.4.4 Achievement of outcomes
The Victorian Government Aboriginal Affairs Report 2013 details the government's progress towards achieving the targets established in VAAF. The reported results contained in Appendix C, demonstrate that — despite the development of programs aimed at increasing access in order to close the gap between Aboriginal people and the rest of the population — there is limited evidence of the gap being closed. For example, the gap between rates of Aboriginal and non-Aboriginal youth being held in detention, and in rates of kindergarten access remained wide in 2012. In many cases the gap appears to have widened, such as in child protection and literacy and numeracy.
Although some data used is more complete than ABS data, in many cases the data used to calculate participation rates is from the ABS. Both ABS and other researchers have found an undercount in census data, which means it is possible that the gap between the Aboriginal and non-Aboriginal populations is greater than that represented in official documents. Departments need to improve the completeness of data in order to gain a better understanding of whether outcomes are being achieved, and accurately report on progress toward targets.
DH aside, departments are not undertaking evaluation or setting outcome-based targets that would enable an understanding of whether or not improvements are being made. The absence of evaluation means that departments cannot be assured their programs are effective and efficient or know the extent to which they are contributing to outcomes.
DEECD conducts some evaluations but does not have outcome-based targets against which it can measure progress. DEECD provided evidence that it analyses three‑year‑old kindergarten participation rates as part of its Early Start Kindergarten program annual reporting but provided no evidence that it is analysing four-year-old kindergarten participation rates, although it reports against them. This is important because one of the headline closing the gap targets in VAAF relates to four-year-old kindergarten. DEECD also uses the Australian Early Development Index, which is a full population census of children in their first year of schooling relating to health and wellbeing outcomes. Although this is a useful tool, it is high level and does not directly assess outcomes related to specific DEECD programs and services considered as part of this audit.
While DHS conducts evaluations, the majority of these do not specifically relate to Aboriginal access. DHS provided evidence that it measures access to public housing and homelessness services, but it is not clear how this data is used or if it is interrogated to ensure demand is being met.
The government's progress towards achieving the targets established in VAAF is located in Appendix C. These results indicate that departments will have to overcome some significant gaps to achieve key VAAF targets and outcomes, although there are improvements in some areas such as kindergarten and MCH participation.
While MCH participation rates had increased over the previous five years and the gap had narrowed, in 2012–13 participation decreased and the gap widened again at all stages except the two-year-old visit. Despite this, participation in the MCH service has increased for Aboriginal Victorians since 2006–07. The benefits of attending the MCH service can include reduced child mortality, increased birth weight, and the opportunity for early intervention for issues. This means that increased participation in the MCH service is positive in itself.
Perinatal mortality and birth weight rates involve a very small population and although the trend appears to be improving, results are very sensitive to fluctuation. However, some outcomes are worsening — for example, rates of presentations to emergency departments for self-harm incidents have doubled since 2005.
The VAAF target relating to kindergarten access aims to close the gap between Aboriginal children and rest of the eligible population by 2014. Between 2001 and 2011 Aboriginal kindergarten participation rates increased by 1.8 per cent. In 2012 there was an increase of 11.6 per cent — which brought the Aboriginal participation rate to 81.7 per cent compared to 97.9 per cent for the rest of the population. This meant the gap narrowed by 8.3 per cent to 16.3 per cent between 2011 and 2012, which is the most recent data available. At the current rates of increase, it is unlikely that gaps will be closed in line with targets.
4.5 Monitoring and reporting
Effective monitoring of performance and transparent and accurate reporting are imperative for the Victorian Government to meet its intergovernmental commitment to close the gap. A variety of plans and programs will be necessary to achieve the high‑level targets listed in VAAF. Accurate and transparent reporting is critical to demonstrate that departments are providing equitable access to services in order to meet targets and achieve outcomes across government in line with Council of Australian Governments (COAG) agreements.
All departments have external reporting commitments and various internal reporting processes. DH has a (draft) Koolin Balit performance management framework which sets out reporting arrangements for initiatives under the Koolin Balit strategy. DEECD requires MCH service providers to submit annual service improvement plans, and kindergartens report data collected in the August census week. The DHS Board regularly receives reports detailing progress against key indicators and targets, although we have not been provided with evidence of this.
The Secretaries' Leadership Group on Aboriginal Affairs (SLG), supported by OAAV, is responsible for overseeing the implementation of VAAF. However, this arrangement does not appear to have been effective, and seems to lack the authority required to ensure that VAAF is implemented as intended.
Office of Aboriginal Affairs Victoria
OAAV is responsible for supporting SLG in delivering VAAF and in overseeing the development of departmental Aboriginal inclusion action plans. OAAV monitors outcomes related to Aboriginal Victorians, consistent with government's commitments in VAAF and under the National Indigenous Reform Agreement, and also has responsibility for coordinating and delivering the annual Victorian Government Aboriginal Affairs Report.
Victorian Government Aboriginal Affairs Report
The Victorian Government is required to report annually on departments' progress towards outcomes for closing the gap between Aboriginal and non-Aboriginal Victorians. OAAV collects information from departments for publication in the annual Victorian Government Aboriginal Affairs Report (VGAAR). However, VGAAR does not provide comprehensive data, just a high-level analysis of outcomes against targets in key areas and some basic data on trends.
Not all targets, progress and other measures are reported against. Examples include:
- Targets relating to closing the gap in employment outcomes are not reported against, because no new data has been made available since 2011.
- There is no target for reducing the incidence of family violence and so progress is not reported.
- The target relating to closing the gap in Year12 attainment is not reported against.
- Targets relating to health status do not have comparable data — i.e. for the same year — to determine if the gap is closing.
- The proportion of Aboriginal Victorians who are homeless is not reported.
- The gap in levels of psychological distress is not reported.
- There are no targets or progress reports against strategic action areasix–Strong culture, engaged people and confident communities.
Reporting under the Victorian Indigenous Affairs Framework
Under the previous whole-of-government framework, targets and measures in the Victorian Indigenous Affairs Framework (VIAF) were reported against in annual Victorian Government Indigenous Affairs reports. However, these reports provided basic information on departments' progress in improving service access. Departments were not required to report against the VIAF and progress against 2013 targets was not reported. As a result, there is no evidence VIAF contributed to improved outcomes.
Victorian Government Budget and Reporting Framework
Departments must include in their annual reports a comparison of output targets specified in State Budget Paper No.3–Service Delivery (BP3) with actual performance against those targets. In BP3 and departmental annual reports there is no detailed reporting specifically related to outcomes for delivery of services to Aboriginal people. Performance measures for DEECD are limited to literacy and numeracy at school, DH has no performance measures for its Aboriginal services programs and DHS has only two, which are related to family services and the placement of Aboriginal children with relatives and carers.
Although departments report on results of their various programs in addition to BP3 targets, there is significant scope for improved public reporting on the accessibility and outcomes of mainstream services for Aboriginal Victorians.
Public reporting
Reporting on whether access has improved and outcomes are being achieved should be transparent, and reporting on participation rates should be on the proportion of a population that is accessing a service so that it is clear if there has been progress in closing the gap. The Aboriginal population growth rate is higher than that of the rest of the population, and this coupled with an increased willingness to identify, has led to sharp increases over the past 10 years in the number of identified Aboriginal Victorians. This means that in many cases the number of Aboriginal Victorians accessing a service has increased significantly, but the increase in identified population, coupled with birth rates and migration, means that the proportion accessing a particular service may not have changed. This is important because the way that data is reported is key to understanding progress towards closing the gap targets.
All of the audited departments report in some capacity to several state and Commonwealth organisations including:
- Productivity Commission — Report on Government Services, Indigenous Compendium, Indigenous Expenditure Report
- Commonwealth Government departments — including the Department of Education, Department of Health and Department of Social Services
- COAG.
DH published the final report of the evaluation of its Closing the Gap in Aboriginal Health Initiative. This was a comprehensive report delivering mixed results. On its website, DEECD publishes the MCH service annual report, containing data relating to attendance at 'key ages and stages visits'. While this is a positive step, the report consists largely of figures, with no commentary or analysis, and does not discuss whether the intended outcomes of the service are being achieved. DHS has not conducted comprehensive evaluations of its major Aboriginal plans, programs and strategies, and does not have this information available.
4.5.1 Funding of services
Quantifying the Victorian Government's expenditure on mainstream services for Aboriginal Victorians is difficult. This appears particularly so for DHS. The total budget for DHS service delivery for all Victorians in 2012–13 was $3.6 billion and included $1.5 billion for disability services and $400 million for housing assistance. However, DHS was unable to provide specific funding details on access of these mainstream services by Aboriginal Victorians. DHS advised that it does not fund mainstream service providers for specific cohorts of clients — it prioritises access to mainstream services based on need, enabling a variety of vulnerable cohorts to access services.
In 2012–13, DEECD spent around $65 million on its various programs for Aboriginal Victorians, and it provided specific funding details for each of its Aboriginal programs. However, it was not able to provide specific expenditure for Aboriginal Victorians in the MCH service.
DH spent $49 million in 2010–11 on its Aboriginal health programs and services, which increased to $62 million in 2012–13.
Although OAAV is the central policy group for Aboriginal affairs, it was unable to provide any information on the amount of funding for programs related to services for Aboriginal people across Victorian Government departments.
In our June 2008 report, Coordinating Services and Initiatives for Aboriginal People, we noted that the former Department of Planning and Community Development (DPCD) recognised that investment in Indigenous affairs had been ad hoc, short term and not always appropriately directed for sustained improvement. DPCD identified the need for an 'investment map' that outlined the funding requirements for the previous VIAF. Since that report, little progress has been made to clarify the resource needs for achieving the government's long-term goal of closing the gap between Aboriginal and non-Aboriginal Victorians.
Departments should consider developing an investment map, which shows the funding requirements over the term of the government's commitment to VAAF, and how the spending will match patterns of need.
4.5.2 Governance arrangements
SLG supported by OAAV is responsible for overseeing the implementation of VAAF. The terms of reference for SLG include:
- oversight of the implementation of VAAF 2013–15 and ensuring integration of effort across departments
- providing advice on appropriate investment towards closing the gap in outcomes between Aboriginal and non-Aboriginal Victorians
- monitoring and evaluating progress to ensure achievement against COAG and key state indicators
- oversight of the implementation of the government's inclusion framework to improve access by Aboriginal people across service systems
- ensuring COAG strategies are implemented in a coordinated manner that maximises benefits for Aboriginal Victorians
- providing advice on and oversight of Aboriginal community engagement processes to ensure that these processes effectively reflect the views of Aboriginal Victorians.
The terms of reference require SLG to hold at least three meetings each year with key departmental secretaries. Examination of minutes indicates SLG does not actively monitor VAAF implementation by departments. We noted that SLG:
- approved the Victorian Government Aboriginal Affairs Report 2012
- considered the findings of the 2013 OAAV-initiated preliminary review of departmental Aboriginal inclusion action plans.
While the terms of reference outline the oversight role of SLG, it and OAAV appear to lack the executive authority to directly influence departments in the development and implementation of their plans. OAAV emphasised that the departments are responsible for developing and implementing their own plans, while OAAV is responsible for coordinating the annual Victorian Government Aboriginal Affairs Report. However, VAAF states that oversight will be led by SLG and will drive the development of departmental Aboriginal action inclusion plans to ensure services are accessible and inclusive for Aboriginal Victorians.
According to OAAV, its role involves influencing and facilitation, rather than the authority to direct the way that departments undertake their work. However, OAAV does not verify the information provided by departments or audit data collection processes, nor does it or SLG monitor the funding arrangements and departmental budgets for Aboriginal service delivery.
Lack of effective action over time
Numerous findings in this audit reflect similar issues identified in our June 2008 report Coordinating Services and Initiatives for Aboriginal People, which, among other things, found:
- draft action plans under the former VIAF did not address core requirements — in many instances these plans were never completed
- funding commitments were not matched to the scope and longevity of Indigenous needs
- data limitations meant that it was not possible to undertake robust assessments of progress against VIAF's outcomes.
The 2008 report noted that many issues raised in previous reviews dating back to 2002 had not been addressed and recommended that roles, responsibilities and accountabilities needed to be clarified — particularly those of oversight bodies such as the then Ministerial Taskforce for Aboriginal Affairs and the SLG. The report noted that greater clarity of responsibilities would improve the administration and facilitate alignment with a 'joined-up' approach to service delivery.
An absence of effective leadership and oversight has adversely affected the delivery of mainstream services for Aboriginal Victorians over many years. There is limited public accountability despite the existence of whole-of-government arrangements, such as the SLG, under both VAAF and the previous VIAF. Given the lack of oversight it is unclear what is expected of departments in Aboriginal service delivery and unclear if departments intend, in the main, to fully apply the principles and criteria detailed under VAAF.
Given the deficiencies identified in this audit, such as with Aboriginal action plans and strategies; data collection, coordination, collaboration and sharing; and program evaluations, SLG and OAAV need to provide more active leadership, direction and oversight to make sure that departmental programs and strategies facilitate increased access and improved outcomes for Aboriginal Victorians.
Recommendations
That departments:
- routinely evaluate plans and programs to determine whether access is increasing and outcomes are improving, and to identify where improvements are needed
- develop internal and external reporting regimes that provide comprehensive and informative data on the progress and outcomes of departmental plans and programs.
That the Department of Premier and Cabinet:
- provides more active leadership and direction so that departmental programs and strategies align with the Victorian Aboriginal Affairs Framework 2013–18, and identifies and addresses increased access and improved outcomes
- through the Secretaries' Leadership Group on Aboriginal Affairs, monitors the implementation of departmental plans, evaluates outcomes and monitors the development of investment logic maps that identify the funding requirements over the term of the government's commitment to the Victorian Aboriginal Affairs Framework 2013–18.
Appendix A. Barriers to access and required actions
Introduction
Figure A1 lists the barriers to mainstream services for Aboriginal Victorians and the actions required to address them.
Figure A1
Barriers and required actions
Barriers |
Required actions |
|---|---|
Lack of culturally safe services — services may not be culturally safe or properly equipped to manage the cultural needs of Aboriginal people. Staff may not possess the required expertise. |
Cultural awareness training and equipment that is reflective of the cultural needs of Aboriginal people in the local area, as well as statewide. |
Awareness of the services that are available — services may not be visible, and low literacy levels among the population mean that some people are reliant on word of mouth. |
Improvements in visibility and coordination across services — including visibility of services to service providers — to ensure that Aboriginal people are aware of services they are entitled to access. |
Lack of required services in the local area — for example, detox and rehabilitation services in the Goulburn Valley. Visibility of available services in this area is an issue that was also raised by Mildura stakeholders. |
Improvements in communication of services that are available as well as consideration of expanding services into areas of need. |
Racism — this appears particularly pronounced in the private housing market. This has a negative impact on homelessness levels. |
Cultural awareness training and flexibility within services to adapt to needs. |
Lack of transport to service delivery points — particularly in regional areas, transport to services is a problem. Consultation with early childhood providers indicated that lack of transport prevents attendance at maternal and child health care checks and at kindergarten. |
Improvements to transport options, including provision of transport to kindergarten and maternal and child health services, or expanded outreach services. |
Shame/embarrassment/fear — emanating somewhat from parents with low literacy levels and/or older generations. There is a pervasive fear of government that prevents people from accessing services, or influences their perception of a service. |
Ensure that services are culturally safe and visible, including to people who may be illiterate. |
Administrative processes — especially filling out complex forms. For some Aboriginal people access to services is far too onerous. |
Reduce onerous requirements for forms. |
Transience — many families are transient and children may have never had their birth registered. Discussions with stakeholders and service providers indicate that children may not be registered at birth and therefore an indeterminate number of Aboriginal children are not known to services and 'fall through the cracks'. |
Better coordinate services so that hospitals can assist in registering births and maternal and child health services can engage in outreach. Improve data and engage in outreach across all departments to quantify the extent of the problem and ensure access to services is provided. |
Affordability — in many cases bearing any cost at all prevents accessing services. |
Ensure that all costs of accessing services are considered, including transport, accommodation and other costs. |
Inadequate funding of services — services cannot provide the required outreach or additional support that ensures eligible people receive the service. |
Ensure that services have the flexibility in funding required to ensure eligible people are able to access the service. |
Source: Victorian Auditor-General's Office.
Appendix B. Mainstream services, strategies and programs
Figure B1 sets out the service responsibilities of audited departments and their recent strategies, plans and related documents that are relevant to accessibility of those services to Aboriginal Victorians.
Figure B1
Audited department services, strategies and programs
Mainstream services |
Strategies/related documents |
Additional programs and services designed to assist access |
|---|---|---|
Department of Human Services |
||
Disability Housing and homelessness |
|
|
Department of Health |
||
Health:
Mental Health:
Aged Care:
|
|
Programs with Aboriginal Victorians as a specific target group, among others:
|
Department of Education and Early Childhood Development |
||
Kindergarten Maternal and child health service Parenting Services |
|
|
Source: Victorian Auditor-General's Office.
Appendix C. Progress toward targets
Introduction
Figure C1 sets out progress toward targets and other measures as detailed in the Victorian Aboriginal Affairs Framework 2013–18.
Figure C1
Progress towards Victorian Aboriginal Affairs Framework targets
Maternal and early childhood health and development |
||
|---|---|---|
Headline indicator |
Targets |
Progress toward targets |
Improve Aboriginal infant survival and health |
By 2023, close the gap in the perinatal mortality rate. |
Perinatal mortality rate per 1 000 births increased from 13.3 in 2005 to 20.4 in 2009 and decreased to 10.7 in 2011 — this is the lowest level since 2004. Perinatal mortality rate for babies born of non‑Aboriginal mothers declined from 8.2 to 6.8 over the same period. |
By 2023, close the gap between Aboriginal and non‑Aboriginal babies with a birth weight below 2 500 grams. |
There are significant fluctuations in birth weight rates, but since 2004, the proportion of babies born to Aboriginal mothers with low birth weight has decreased from 16.2 per cent to 13.1 per cent in 2011. Rates of low birth weight were 12.1 per cent for Aboriginal babies and 6.8 per cent for non‑Aboriginal babies in 2011. |
|
Increase Aboriginal kindergarten participation |
By 2014, the gap between Aboriginal and non-Aboriginal four-year-old children having access to a high quality kindergarten program will be closed. |
In 2005, the participation rate was 66.4 per cent, with a gap of 26.3 per cent. In 2012, the participation rate increased to 81.6 per cent, with a gap of 16.3 per cent. |
Reduce the rate of Aboriginal child protection substantiations |
By 2023, the gap in the rate of Aboriginal and non-Aboriginal child protection substantiations will be reduced by 75 per cent. |
The gap has widened in recent years. In 2009–10 the rate per 1000 for Aboriginal children was 46.9 and for non-Aboriginal children, 4.7. In 2012–13 this was 67.4 and 7.2 respectively. |
Other measures |
Current progress on other measures |
|
|
|
|
|
|
|
|
|
|
Education and training |
||
|---|---|---|
Headline indicator |
Targets |
Progress toward targets |
Improve literacy and numeracy in Years 3, 5, 7 and 9 for Aboriginal students |
By 2018, halve the gap for Aboriginal students in reading, writing and numeracy. |
Between 2008 and 2013, gaps widened in Year 3 reading, writing and numeracy, from 3.8 to 7.8 per cent, 5.3 to 7.6 per cent, and 3.8 to 7.8 per cent respectively. In Year 5, the gap in reading narrowed from 11 to 5.4 per cent, but gaps in writing and numeracy widened from 11.4 and 11.7 per cent to 12.1 and 9.1 per cent respectively. In Year 7, the gap in reading narrowed from 10.6 to 9.7 per cent, but the gap in writing and numeracy widened from 18.1 and 8.9 per cent to 19 and 9.9 per cent respectively. In Year 9, the gap in reading narrowed from 15.1 to 10.8 per cent, the gap in writing widened from 21.3 per cent to 22 per cent, and the gap in numeracy narrowed from 17.1 per cent to 16.8 per cent. |
Increase the proportion of Aboriginal young people aged 20–24 who have completed at least Year 12 or equivalent. |
By 2020, halve the gap between the Year 12 or equivalent attainment rates of Aboriginal and non‑Aboriginal 20–24 year olds. |
Victorian Government Aboriginal Affairs Report reports the number of Aboriginal students completing Year 12 or equivalent as increasing from 127 in the school sector and 44 in the vocational education and training sector in 2002 to 380 in 2013 but does not actually report the gap in attainment. It therefore does not report on this target. |
Other measures |
Current progress on other measures |
|
|
|
|
|
|
|
|
|
|
|
|
|
Economic participation | ||
|---|---|---|
Headline indicator |
Targets |
Progress toward targets |
Increase Aboriginal labour force participation |
By 2018, halve the gap in employment outcomes between Aboriginal and non‑Aboriginal Victorians, as measured by:
|
In 2011, approximately 48 per cent of Aboriginal Victorians aged 15 and over were employed — no new data or trending on this was provided to determine if the gap is closing. Aboriginal unemployment is 19 per cent, and the labour force participation rate has remained steady. |
Increase workforce participation by Aboriginal people in the public sector |
By 2018, employment of Aboriginal people in the Victorian public service will increase to 1 per cent of total employees. |
The employment rate was 0.7 per cent in 2010 and 0.8 per cent in 2013. |
Other measures |
Current progress on other measures |
|
|
|
|
|
|
|
Health, housing and wellbeing |
||
|---|---|---|
Headline indicator |
Targets |
Progress toward targets |
Improve the health status of Aboriginal Victorians |
By 2031, close the gap in the proportion of Aboriginal and non‑Aboriginal Victorians that report their health status as 'excellent or very good'. |
In 2012–13, 40.3 per cent of Aboriginal Victorians reported their health to be 'excellent or very good'. No comparable data was provided from the same source, but in 2011–12 58.9 per cent of all Victorians reported their health as 'excellent or very good'. |
By 2031, close the gap between Aboriginal and non‑Aboriginal adults reporting 'high or very high' levels of psychological distress. |
No comparable data was provided, but 32.3 per cent of Aboriginal Victorians report experiencing high or very high levels of psychological distress. |
|
By 2023, reduce the proportion of Aboriginal adults who are smokers to 21 per cent. |
The same survey reported 39.7 per cent of Aboriginal Victorians aged 15 years and over smoked daily. No comparable data was provided, but the rate for all Victorians in 2011–12 was 15.6 per cent. |
|
Other measures |
Current progress on other measures |
|
|
|
|
| |
||
|
|
|
|
|
|
||
|
|
|
|
Safe families and communities and equitable justice outcomes |
||
|---|---|---|
Headline indicator |
Targets |
Progress toward targets |
Reduce the incidence of Aboriginal family violence |
Further work is required to develop an appropriate target. |
n/a |
Reduce the over‑representation of Aboriginal people under justice supervision |
By 2031, close the gap in the rate of Aboriginal and non‑Aboriginal people under youth justice supervision. |
In 2012–13, 16.79 per 1 000 Aboriginal young people were on a community based order, compared to 1.12 non-Aboriginal young people, an increase from 15.2 and 1.26 respectively in 2007–08. Although the figure for Aboriginal young people reached 20.48 in 2010–11 and has decreased since then, the gap has widened. Over the same time period the rate of Aboriginal and non-Aboriginal youth in detention declined from 2.18 to 1.16 and 0.1 to 0.09 per 1 000 respectively. From 2005–06 to 2012–13, the gap widened, with Aboriginal people in 2012–13 under supervision at a rate of 38.6 per 1000, compared with 2.9 per 1000 for the rest of the population. |
Reduce the proportion of Aboriginal people who return to prison within two years of release |
Since 2005–06, the proportion of Aboriginal people who return to prison within two years of release has decreased from 56.5 per cent to 50.3 per cent. |
Safe families and communities and equitable justice outcomes–continued |
Other measures |
Current progress on other measures |
|
|
|
| |
|
|
| |
|
|
| |
|
|
| |
Strong culture, engaged people and confident communities |
||
|---|---|---|
Headline indicator |
Targets |
Progress toward targets |
Strengthen Aboriginal culture and support Aboriginal people's engagement with community and society |
None |
n/a |
Other measures |
Current progress on other measures |
|
|
|
|
|
|
|
|
|
|
|
|
|
(a) The percentage is greater than 100 per cent because it is calculated as a percentage of their respective cohort at the commencement of their secondary schooling at year 7. Because of student movements over the period, the figure may exceed 100 per cent.
Source: Victorian Auditor-General's Office based on Victorian Government Aboriginal Affairs Report 2013.
Appendix D. Audit Act 1994 section 16—submissions and comments
Introduction
In accordance with section 16(3) of the Audit Act 1994, a copy of this report was provided to the Office of Aboriginal Affairs Victoria and the departments of Education and Early Childhood Development, Health, and Human Services.
The submissions and comments provided are not subject to audit nor the evidentiary standards required to reach an audit conclusion. Responsibility for the accuracy, fairness and balance of those comments rests solely with the agency head.
Responses were received as follows:
-
Collaborative response provided by the departments of Premier and Cabinet, Education and Early Childhood Development, Health and Human Services.
Collaborative response provided by the departments of Premier and Cabinet, Education and Early Childhood Development, Health and Human Services.