Residential Care Services for Children
Overview
On any given day around 500 children are in residential care in Victoria. These children are among the most vulnerable in the community. They are generally in the Out of Home Care system because they are at risk of harm, abuse or neglect from their families. The children are placed under the protection of the Secretary of the Department of Human Services. Residential care, which involves placing a small number of children or young people in a home in the care of paid staff, is often considered a placement option of last resort.
The audit found that the residential care system has insufficient capacity and capability to respond to the level of demand and growing complexity of children’s needs. This affects the quality of care provided and reduces opportunities for children to achieve positive outcomes while in care. Current staffing models do not provide sufficient quality and stability of care for children. This has implications for the children’s health, education and other outcomes. Children have better outcomes in the therapeutic residential care model, which has planned placements and staff access to a therapeutic specialist, than in the standard model of care.
Residential Care Services for Children: Message
Ordered to be printed
VICTORIAN GOVERNMENT PRINTER March 2014
PP No 304, Session 2010–14
President
Legislative Council
Parliament House
Melbourne
Speaker
Legislative Assembly
Parliament House
Melbourne
Dear Presiding Officers
Under the provisions of section 16AB of the Audit Act 1994, I transmit my report on the audit Residential Care Services for Children.
The audit examined the effectiveness of the Department of Human Services' residential care services for children and young people. The audit assessed whether children's needs for safety, stability and personal development are being met and whether the residential care system is subject to effective oversight and review.
I found significant shortcomings with respect to these issues. The system has insufficient capacity and capability to respond to the level of demand and growing complexity of children's needs. This affects the quality of care provided and reduces opportunities for children to achieve positive outcomes while in care.
I have made a series of recommendations aimed at strengthening the system, improving the quality of service provision and meeting the needs of children in residential care. I am encouraged by the Department of Human Services' stated commitment to implement actions against all six recommendations.
Yours faithfully
John Doyle
Auditor-General
26 March 2014
Auditor-General's comments
 John Doyle Auditor-General |
Audit team Michele Lonsdale—Sector Director Kate Sullivan—Team Leader Melinda Gambrell—Analyst Andrew Evans—Engagement Quality Control Reviewer |
Auditor-General's comments
A society is measured by how it treats its most vulnerable members. Children in residential care are among the most vulnerable people in our community and their interests are not being well served.
Children in residential care are likely to have suffered significant neglect or abuse in the family home. Often they experience the additional trauma of being placed in a unit with a group of similarly traumatised children. Without appropriate care and support the future for many of these children is bleak.
One of the more disturbing issues, which has attracted media attention, is the risk of sexual exploitation of children in residential care. This is but one of many serious issues symptomatic of a system failing to find effective answers to what is clearly a difficult, complex set of social policy challenges. Regrettably, there has been a fundamental failure to oversee and ensure the safety of children in residential care.
There is a considerable onus on the state and on the residential care providers it funds to provide for children’s physical, intellectual, emotional and spiritual development in the same way a good parent would.
Being ‘a good parent’ means keeping children in safe, stable circumstances where their wellbeing, educational and health needs can be met, and where they can be given the life skills to live independently and productively after leaving care. Providing for these levels of service is challenging. But the risks of not doing so are quite unacceptable, both for the children themselves and for any caring community.
For residential care services to be effective there needs to be strong and effective oversight, a primary focus on improving outcomes for children, well-trained and appropriately qualified staff, and ongoing monitoring and review to enable continuous improvement.
My office has examined each of these aspects of Victoria’s residential care services for children and found significant shortcomings.
Each year the Department of Human Services (DHS) knows that around 500 children will require residential care, yet it does not plan for this number. Consequently, the department relies heavily on contingency funding and funding that has been earmarked for other DHS initiatives.
My audit has identified a gap in independent advocacy for individual children. This is of concern because the children in residential care often do not have families who can take on this role. They need someone who can listen to their concerns about what is happening to them and advocate on their behalf.
I am encouraged by DHS’s stated commitment to actions against each of my recommendations but am unclear as to when the community can expect to see the fundamental issues addressed. DHS has developed a five-year Out of Home Care plan which, at the time of finalising this report, was yet to be finalised and released. Any future plan will need to sufficiently address the fundamental systemic failures identified by my audit and have specific actions and completion dates. I intend to revisit the issues that my office has identified to ensure they are being appropriately addressed.
John Doyle
Auditor-General
March 2014
Audit Summary
There are currently around 500 children in residential care in Victoria. These children are among the most vulnerable in the community. They are in the Out of Home Care (OOHC) system because in most cases the Children's Court has decided they are at significant risk of harm, abuse or neglect from their own families and cannot remain in the home. The Children's Court places these children under the protection of the Secretary of the Department of Human Services (DHS).
Residential care is one of three main OOHC placement options available to the Secretary. DHS's preferred options are kinship and foster care. Residential care is the most expensive option, requiring 24-hour care by paid staff for a small group of children in a residential unit or house. DHS funds community service organisations (CSO) to provide the placement services for children.
Children in residential care have complex needs relating to mental health, cognitive development and social interaction. They are likely to engage in extreme behaviours, such as self-harm, aggressive or sexualised behaviours, substance abuse and other activities that place them, or others, at high risk. They feature in a disproportionate number of critical incidents when compared with other at-risk children in OOHC. For Aboriginal children there is the added impact of past government policies, discrimination and intergenerational trauma.
Figure A
Common characteristics of children in residential care
|
Children in residential care have generally been exposed to multiple traumas in the form of family violence, alcohol and drug abuse, or sexual, physical and emotional abuse since they were very young. They may have a parent who is in prison or a struggling single parent with mental health issues. Some have been born to mothers who were very young, often with a violent partner. They usually have other siblings in care, and one of their parents may also have been in care as a child. They are usually known to child protection at an early age. They come to residential care typically as a young adolescent, having experienced a number of placements in home-based care that have since broken down or were only available for short periods of time. They often come to residential care with little warning and with few belongings. On their 18th birthdays, if not before, they leave the protection of the state. |
Source:Victorian Auditor-General's Office based on case file analysis.
A child will be placed in residential care if they cannot stay in other home-based placement options either because their needs are too great or because the kinship or foster care options are not available or cannot keep them safe. Residential care is often an option of last resort.
DHS is responsible for protecting these children from harm. Under the Children, Youth and Families Act 2005 the Secretary of DHS acts as custodian or guardian for the vast majority of children in residential care, and is responsible, when placing a child in care, for providing for 'the physical, intellectual, emotional and spiritual development of the child in the same way as a good parent would'.
The challenges involved in ensuring that the children are in safe and stable placements which meet their health and education needs, encourage positive family and cultural connections, and prepare them for independent living are widely acknowledged. The costs to the child and community of not achieving these outcomes are high.
Outcomes for many of the children in residential care are bleak due to the considerable trauma they have already experienced in their lives and the impact this trauma has had on their physical and mental wellbeing and developmental needs. It is critical that the system is effective and efficient and able to meet the children's significant needs.
This audit focused on DHS's oversight of residential care services and the outcomes for children in the residential care system. The audit team visited six CSOs funded by DHS to provide residential care services and one DHS-operated residential care service. These providers collectively had 157 children in their care as at 30 June 2013, representing around 31 per cent of all children in residential care. The audit did not examine kinship care or foster care placements.
Conclusions
The residential care system is unable to respond to the level of demand and growing complexity of children's needs. It has been operating over capacity since at least 2008. DHS is paying a premium to place children in residential care outside the planned capacity of the system.
The lack of sufficient capacity affects the quality of care provided and reduces opportunities for children to achieve positive outcomes while in care. Because of system constraints, decisions about where a child should be placed are not always able to be made in the child's best interests. This puts at risk efforts to protect the child from harm, protect their rights and promote their development.
The outcomes for children in residential care, particularly in the standard model, are poor across a range of indicators, including health and education. This reflects the transience of staff, their lack of qualifications, skills and training, and the level of support provided to them. The therapeutic residential care model shows better outcomes for children than the standard care model, largely because it builds staff capability.
There is no independent advocacy on behalf of individual children in residential care. This is a critical gap, given that many of the children do not have families to advocate on their behalf.
Findings
The system is operating over capacity
In the past 10 years, the number of children in OOHC has increased by 60 per cent, while the number of children in residential care has grown by 10 per cent during the same period. The needs of the children in residential care are becoming increasingly complex. On average, children are also staying longer in residential care. These trends have placed considerable pressure on the system.
In 2012–13, DHS planned for 459 residential care placements. However, on any given day in 2012–13, an average of 508 children were in residential care placements, meaning the system was operating over capacity. Insufficient capacity affects the quality of care children receive. For example, placement decisions are often based on bed availability, rather than on matching the needs of highly vulnerable children with the needs and behavioural characteristics of the children who are already in residential care units. Poor placement can lead to an incompatible mix of children in a residential unit, with implications for safety and children's ability to achieve positive outcomes.
DHS efforts to reduce the overall demand for residential care places through diversion strategies have been only partially successful. While there are more children in kinship care, the number of children in foster care is declining because there are fewer foster carers available. DHS has been successful in reducing the number of children under the age of 12 in residential care but this has resulted in a more concentrated mix of older children with more entrenched behaviours and complex needs.
Residential care costs are significant
The total cost of funded residential care services annually is over $100 million. In 2013–14, the annual cost of a residential care placement ranges from $162 880 to $308 028.
Operating over capacity means that DHS must purchase additional capacity to meet the demand for residential services. In 2012–13, DHS purchased additional placements at a cost of $24 million. The funding for these placements came from other DHS programs. DHS is paying additional costs to place children in residential care outside the planned capacity of the system.
The key driver of individual placement cost is client complexity. Placements for some children with significant and extreme needs cost close to $1 million for a year.
In 2008, DHS piloted the therapeutic residential care model. Currently, 80 placements have been funded under this model. CSOs delivering a therapeutic placement receive a loading of $74 580 on top of their current funding level to provide the service, which includes additional resources such as a therapeutic specialist.
Performance monitoring is inadequate
DHS does not systematically monitor outcomes for the whole residential care population. CSOs are required to report only outputs, not outcomes.
Record-keeping practices and case plan implementation and monitoring are not subject to sufficient and appropriate quality assurance mechanisms.
DHS's incident reporting system, which is an important means of identifying and responding to risks to children's and staff safety, is time consuming to use and inefficient. The client relationship information system (CRIS), which has an extensive range of functions including recording client information and supporting service providers in case management, is cumbersome and disorganised. Manual handling of critical information raises questions about its reliability.
Staff capability needs to be strengthened
Current staffing models are not providing sufficient quality and stability of care for children in residential care, with implications for children's education, health and other outcomes. No formal qualifications are required to work in residential care services, yet staff are employed to care for children with complex needs, including violent and risk‑taking behaviours, substance abuse and mental health issues. With casual staff making up 55 per cent of the residential care workforce, staff transience and a heavy reliance on temporary labour reduces stability for children.
A key feature of the therapeutic residential care model is the availability of a specialist to work with residential care staff to build confidence and expertise to manage children's needs and challenging behaviours. This contributes to the better outcomes achieved for children in therapeutic residential care placements.
Children's needs are not always being met
Children in residential care generally experience poorer outcomes than children in other types of OOHC.
School attendance, health, and preparedness for independent living after leaving care are poor. More than one-third of children and young people in residential care have experienced over 10 OOHC placements. The number of critical incidents, such as death or severe trauma, is disproportionately high for children in residential care compared with children in other forms of OOHC care.
The therapeutic residential care model has been found to have better outcomes than the standard residential care model in health, education, family connection and transition planning. This is because there is planned placement decision-making and additional funding of $74 580 per placement to provide access to specialist support staff. However the therapeutic model makes up only 17 per cent of placements.
Independent advocacy for children is needed
There is no clear independent advocacy on behalf of individual children in residential care. Such advocacy is particularly important for children who cannot rely on their families to provide this support. DHS, the Victorian Ombudsman and CSOs can all receive complaints about care from or on behalf of children in residential care. However, discussions with CSOs and current and former residents showed little awareness of these avenues.
Recommendations
That the Department of Human Services:
- establishes alternative affordable models of care with sufficient flexibility to cater for the varying and complex needs of children
- actively promotes to children in residential care the processes for making a complaint and investigates the feasibility of establishing an independent advocacy role to support children in residential care
- develops performance measures for delivery of residential care services for children to meet legislative requirements and outcomes for children
- ensures that residential care staff have the necessary skills, qualifications, training and support to work effectively with children and their families
- identifies systems and processes for collecting and analysing information which better meet the department's compliance, assurance and reporting needs
- reviews existing demand forecasting approaches and develops plans for the capacity that is actually required.
DHS has committed to a series of actions to address these recommendations. However most of these actions depend on implementation of DHS's five-year OOHC plan which, at the time of finalising this audit, was yet to be finalised and released.
Submissions and comments received
In addition to progressive engagement during the course of the audit, in accordance with section 16(3) of the Audit Act 1994 a copy of this report was provided to the Department of Human Services with a request for submissions or comments.
Agency views have been considered in reaching our audit conclusions and are represented to the extent relevant and warranted in preparing this report. Their full section 16(3) submissions and comments are included in Appendix A.
1 Background
1.1 Introduction
Children placed in residential care are among the most vulnerable individuals in our community. The state has an obligation to make sure that children in the child protection system are in safe and stable environments where they can develop the skills needed to lead independent and productive lives. Studies have found the economic and social costs of not effectively supporting such children are ultimately borne directly by the criminal justice and health systems, and indirectly in the lost productivity associated with poor education levels and homelessness. The personal costs for children who find themselves in need of care through no fault of their own are enormous.
Residential care is often the last resort for vulnerable children needing the state's protection. Children in residential care live in a house or unit with a small number of other children from similarly traumatic situations under the 24-hour care of paid staff.
While the residential care program caters for around 500 children, the substantial level of state investment in the program and its significance for outcomes for children in the care of the state warrant an audit of its effectiveness and efficiency.
1.2 Residential care
A child will enter the Out of Home Care (OOHC) system if the Children's Court decides it is in the child's best interests that they not live with their parent(s), often because of the risk of abuse or neglect. Residential care is one of three main OOHC options for children who are in the child protection system in Victoria. The preferred OOHC placement options of the Department of Human Services (DHS) are two types of home-based care:
- kinship care—with a relative through a formal arrangement
- fostercare—with non-related carers.
Figure 1A shows the main care types.
Figure 1A
Out of Home Care system, 30 June 2013
Source: Victorian Auditor-General's Office based on Productivity Commission Report on Government Services (2014) data.
Residential care is intended mainly for children between the ages of 12 and 17 years, although in June 2013 there were 65 children under the age of 12 years in residential care. A child will be placed in residential care if they cannot stay in either of the other home-based placement options. This may be because the child is part of a sibling group or due to the extreme needs and challenging behaviours of the child, who is likely to have already experienced multiple placements.
The children are often from families that have not been able to provide safe environments, including homes where there has been exposure to parental violence, drug use, mental illness, physical abuse, sexual abuse, or the risk of such abuse.
The children generally have significant and complex problems that may include self‑harm, substance abuse, overtly sexual behaviour, aggression or violence, emotional disturbance, learning disabilities or disorders, and difficulty forming attachments. They may be depressed, anxious, angry, and/or unable to self-regulate their behaviour.
DHS operates two models of residential care—'standard' and 'therapeutic'. Both models provide temporary, short-term or long-term accommodation and support to children who have been removed from the family home. Therapeutic residential care (TRC) is a more intensive model that has similar elements as the standard model but with access to therapeutic specialists and additional staff.
A wide variety of community service organisations (CSO) are funded by DHS to deliver residential care services. Some organisations are quite small and may only provide services to four children in one property. Others are large, are located across multiple divisions and manage multiple residential care placement services. Some CSOs target services to particular groups of children, such as Aboriginal children, sibling groups, adolescents or young mothers.
1.3 Children in residential care
In the past 10 years, the number of children in OOHC has increased by 60 per cent, with the number of children in residential care increasing by 10 per cent over the same period.
Figure 1B provides a snapshot of children living in residential care as at 30 June 2013.
Figure 1B
Children in residential care as at 30 June 2013
|
Of the more than 6 400 children who were in OOHC in Victoria at this time, 504 children were in residential care. Of these:
|
Source: Victorian Auditor-General's Office.
DHS allocates over $100 million per year to 25 CSOs to deliver residential care services on behalf of DHS throughout the state. These CSOs employ over 1 600 staff rostered in shifts to enable around-the-clock care and supervision.
1.4 Legislative roles and responsibilities
The Children, Youth and Families Act 2005 (the Act) provides the legislative basis for protecting children and young people in OOHC, including those in residential care. The role and responsibilities of the Secretary of DHS are specified in Part 4.3 of the Act. As guardian or custodian, the Secretary has the same rights, powers, duties, obligations and liabilities that a natural parent would have.
The Secretary of DHS must consider the principles set out in Part 1.2 of the Act when making any decision, taking any action or providing any service to children. These include the 'best interests principles' and, for Aboriginal children, the 'Aboriginal Child Placement Principle'.
The best interests principles are intended to protect the child from harm, protect their rights, and promote their development. The principles include giving appropriate weight to the child's views and wishes, placing siblings together, and the desirability of continuity and stability in the child's care. The principles place a strong emphasis on the need to consider the impact of cumulative harm and to preserve cultural identity.
Although the best interests principles are not legislatively mandated as a set of 'rights', their application is widely recognised as good practice, and decisions are made within a professional judgement practice model. DHS has articulated these requirements in its child protection practice manual.
The Act requires CSOs providing OOHC services to be registered and to meet quality standards. DHS funds CSOs to deliver residential care services, sets policy and regulates the standard of care. CSOs are responsible for recruiting, assessing, training, supervising and supporting residential carers, supporting children placed in residential care, and taking the lead role in the development and implementation of care plans.
The Commission for Children and Young People Act 2012 established the Commission for Children and Young People to promote continuous improvement and innovation in policies and practices relating to the safety and wellbeing of children, and the provision of OOHC services for children. The commission may conduct an inquiry in relation to a matter affecting the safety or wellbeing of an individual child or group of children but it does not have a complaints-handling role for children.
The Victorian Ombudsman is responsible for investigating and resolving complaints into administrative actions taken by Victorian government departments such as DHS.
1.5 Policy context
In 2002, DHS developed An Integrated Strategy for Child Protection and Placement Services. Among the initiatives subsequently implemented, the Looking After Children best practice framework enables assessment of seven developmental domains, case planning with a strong focus on wellbeing and the shift to a more therapeutic model of care. The OOHC and residential care issues identified in DHS's 2002 integrated strategy remain largely the same today—escalating and changing demand pressures and growing client complexity.
DHS has recently developed a new integrated five-year OOHC plan in response to a recommendation from the 2012 Report of the Protecting Victoria's Vulnerable Children's Inquiry.
Current work on the National Standards for Out-of-Home-Care will see the development of an indicator of 'a sense of security'. This will identify the proportion of children in OOHC who feel safe and secure in their current placement. Full implementation of these national standards, which address a range of indicators, is expected by 2016.
1.6 Reviews and inquiries
Systemic failures have been documented through 30 years of reviews. These reviews include the 1984 Carney Report, the Fogarty Reports in 1989 and 1993, and the 2009 and 2010 investigations by the Victorian Ombudsman. These reviews have consistent themes and findings relating to pressures on the Victorian OOHC system and the need for significant reform.
While the statutory child protection and OOHC systems have been the subject of review, there has been little focus on residential care services specifically. Nevertheless, the recommendations arising from these reviews have clear applications for the residential care context.
In its report investigating the impact of abuse and neglect on children, the recent Protecting Victoria's Vulnerable Children Inquiry identified the need for 10 major system reforms. These included:
- aligning OOHC funding to a child's needs
- clearer departmental and agency accountability for addressing the needs of vulnerable children, in particular health and education
- a strengthened regulatory and oversight framework
- asector-wide approach to professional education.
The 2009 and 2010 Ombudsman reports into DHS's child protection program and OOHC contained 41 (of 42) and 21 recommendations for DHS, respectively. The 2010 Ombudsman's report into OOHC recommended:
- a greater level of scrutiny and transparency to the OOHC program
- the provision of training to child protection and CSO staff on the new guidelines for responding to care concerns in OOHC
- the development of models for projecting future resource demands for the OOHC system 'that provide greater opportunities for ensuring demand is met through planned capacity increases rather than ad hoc arrangements'.
DHS advised that it has implemented all 41 recommendations made to the department in the 2009 report and implemented 17 of the 20 recommendations from the 2010 investigation, with action still being taken on the three remaining recommendations regarding carer reimbursements and client on client abuse.
1.7 Audit objectives and scope
The audit examined the effectiveness of DHS's residential care services for children and young people by assessing whether:
- children and young people are in appropriate residential care services that meet their needs, including safety, stability, and personal development
- theresidential care service system is subject to effective oversight and review.
The audit focused on DHS's planning, monitoring and oversight activities for residential care services. It included site visits to a sample of seven residential care services, which included six CSOs funded by DHS and one DHS-operated residential care service.
Kinship care and foster care placements were excluded from this audit.
1.8 Audit method and cost
DHS and CSOs were key sources of information for this audit. The audit team gathered evidence by:
- conducting interviews with, and reviewing documents provided by, DHS staff from central and divisional offices
- undertaking site visits to a sample of residential care services
- reviewing 28 randomly selected DHS case files for children and young people currently in a residential care placement
- conducting two focus groups with young adults (between 18 and 21 years) who recently left residential care and one focus group with young people (16years and over) who are currently in residential care. These focus groups were conducted in compliance with section 11B of the Audit Act 1994.
The audit was conducted in accordance with section 15 of the Audit Act 1994 and Australian Auditing and Assurance Standards.
Pursuant to section 20(3) of the Audit Act 1994, any persons named in this report are not the subject of adverse comment or opinion.
The total cost of the audit was $385 000.
1.9 Structure of the report
The report is structured as follows:
- Part 2 examines the effectiveness of the system by focusing on the outcomes for children.
- Part 3 examines the efficiency of the system's design and planning approaches.
2 Outcomes for children
At a glance
Background
The Children, Youth and Families Act 2005 sets out the 'best interests principles' of giving priority to a child's safety, stability and wellbeing; preserving positive family relationships; and promoting cultural and spiritual identity for Aboriginal children.
Conclusion
Children's safety, stability and personal development are compromised by system constraints, such as bed availability, staff transience and inadequate monitoring of overall outcomes. Children placed in therapeutic residential care achieve better outcomes than those placed in standard residential care.
Findings
- One third of children in residential care have experienced over 10Out of Home Care placements.
- The Department of Human Services (DHS) does not collect and analyse sufficient outcomes data.
- Children are not adequately prepared for leaving residential care.
- The availability of a therapeutic specialist builds staff capability and improves outcomes for children.
- DHS's data information systems are cumbersome.
- In 2012, casual staff made up 55 per cent of the residential care workforce.
Recommendations
That the Department of Human Services:
- establishes alternative affordable and flexible models of care to cater for complex needs
- actively promotes to children in residential care the processes for making a complaint and examines the feasibility of establishing an independent advocacy model for children in residential care
- develops performance measures for residential care service delivery
- ensures that residential care staff are appropriately qualified, trained and supported
- identifieshow data collection systems and processes can better meet its needs.
2.1 Introduction
Safe and stable care is particularly important in encouraging a child to develop trust in others, form positive relationships and adapt to changing environments. These factors are linked to increased achievement of personal development outcomes, such as good health, positive family and social relationships, and the development of self-care skills.
The Looking After Children best practice framework has been implemented as a joint initiative of the Department of Human Services (DHS) and community service organisations (CSO). It guides DHS staff and residential care workers in developing plans that meet the identified needs of children.
2.2 Conclusion
The safety and stability of children in residential care is compromised by inadequate monitoring of overall outcomes and system constraints, particularly the demand for beds and transience of staff. This means that many children in residential care are not able to achieve positive outcomes. Children in the therapeutic residential care (TRC) model generally experience better outcomes than children in standard residential care mainly because of planned placement and the availability of a therapeutic specialist to work with staff in TRC residential units.
2.3 Safety
'We get taken from our homes to be safe but are we safe really?'
– former resident
When determining whether a decision or action is in the best interests of the child the Secretary of DHS must always consider the need to protect the child from harm. When a child cannot be placed in home-based care, DHS is responsible for finding the child a placement in residential care. This process is facilitated by the Placement Coordination Unit within DHS, which works with CSOs to agree on a suitable placement.
2.3.1 Placement decision-making
DHS and all CSOs visited during the audit identified poor placement matching as the greatest risk to the safety of children in residential care.
A 2012 ministerial review, by the then Child Safety Commissioner, examined a cohort of 16 young people who had all experienced multiple residential care placements. Ten of the 16 children in the case study had experienced, on one or more occasions, some form of sexual assault, abuse or predatory behaviour by co-residents. One of the children was also subjected to persistent bullying by two older residents. The main reasons given for these incidents were placement incompatibility and staff inexperience in handling challenging behaviours.
Figure 2A lists examples of how demand pressure can lead to incompatible placements with consequences for children's safety and stability.
Figure 2A
Examples of trauma behaviours in residential care
|
An adolescent boy has exhibited violent behaviour. He is currently attending a new school because his original school would not allow him to return. He has bullied and been violent towards other children in the residential unit. |
An adolescent girl has on multiple occasions assaulted staff, caused damage to property, self-harmed and verbally abused community members. Numerous staff have left the unit because of her behaviour. |
An adolescent girl who exhibits sexualised behaviour towards male residents is at risk of being exposed to sex work by associating with others in residential care who are engaging in this behaviour. |
An adolescent girl is currently enrolled in an education program, but there is ongoing concern about regular substance abuse, and at times she has presented as significantly intoxicated. She engages in risk-taking behaviours when she is substance-affected. She has engaged in criminal activity and has outstanding charges to be heard in court. |
An adolescent boy has an acquired brain injury that significantly affects his ability to control his behaviour. He exhibits impulsive, aggressive and threatening behaviours, absconds from care, engages in criminal behaviour and substance use—primarily cannabis, chrome and alcohol. He has limited insight into the level of risk he exposes himself to when engaging in these behaviours. |
Source: Victorian Auditor-General's Office based on unpublished documents from the Department of Human Services.
A 2011 evaluation of the TRC model found that careful management of the mix of children in a home 'promotes and ensures feelings of, as well as actual, safety' and 'facilitates relationships and dynamics that promote progress towards desired outcomes for each young person in the unit'. In the TRC model, placements are planned with children transitioning into the residential units over a number of months, with CSOs making sure that the new person will fit in with the existing children in the house.
Currently, 80 placements receive additional funding to operate under the TRC model, representing only 17 per cent of placements in residential care. Additional funding was committed in the 2012–13 budget for TRC, which will take the total TRC placements to around 30 per cent of residential care placements by 2015.
2.3.2 Critical incidents
'Being safe depends on the other young people in the unit.'
– former resident
Given that they represent only a small proportion of the Out of Home Care (OOHC) population as a whole, around 7.9 per cent in 2012–13, children in residential care generate a disproportionately high number of critical incidents.
DHS defines incidents by severity and type. Category one incidents result in serious outcomes, such as client death or severe trauma, and Category two incidents threaten the health, safety or wellbeing of children or staff.
Evidence shows that children aged 13–18 are involved in significantly more incidents than children in other age brackets. During site visits, CSOs explained that children in residential care will often externalise their trauma as part of the healing process, which differs from wilful acts of aggression and deliberate property damage. However, CSOs are required to report all incidents.
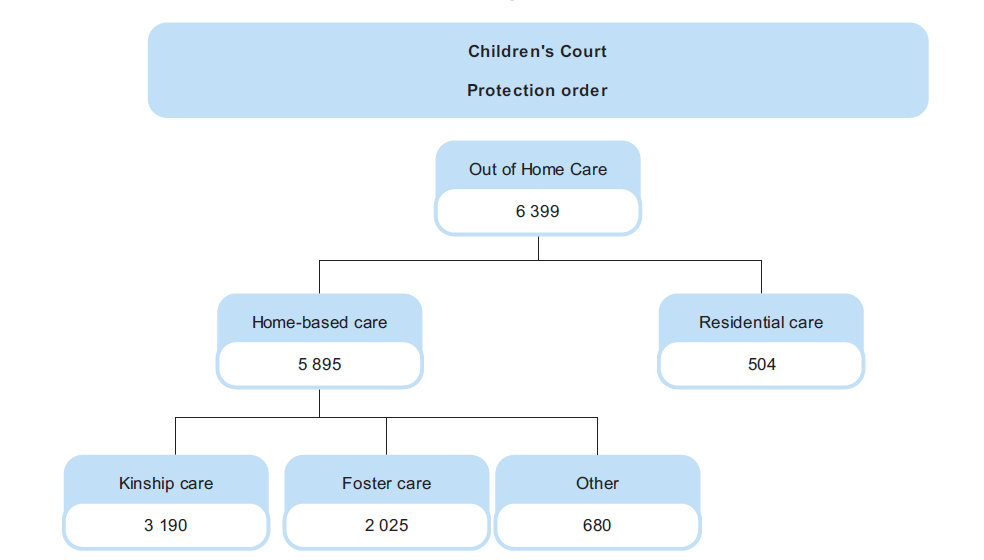
Figure 2B shows the number of Category one incidents in residential care since 2009–10 and the percentage of these incidents out of all OOHC incidents reported. Compared to incidents in the other OOHC categories—kinship and foster care—residential care has the highest number of incidents across all incident types.
Figure 2B
Category one incidents in residential care, 2009–13
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services data.
Figure 2B shows a 49 per cent increase in the number of Category one incidents reported in residential care from 2011–12 to 2012–13. This was mainly due to a marked increase in absent/missing person reports. Missing children are at heightened risk of sexual exploitation. Because absconding can be an indicator of sexual exploitation, DHS has encouraged CSO staff to report all instances of children absent or missing from their units.
Absent/missing person reports include children who were absent from their placement, or whose whereabouts was unknown, or for whom there was grave concern for their or others' safety and welfare. These reports could also be in response to an abduction or kidnapping.
When a child is missing from their placement, the CSO is required to lodge a missing persons report with Victoria Police and to notify child protection through the incident reporting process. Although staff may be aware of a child's whereabouts, they may not be able to immediately look for the child if the staff member is the only person rostered on at that time. Instead, staff will make daily contact by phone to check on the child's safety and encourage the child to return.
Incidents in residential care can also place extra demand on Victoria Police resources. Police may be involved in looking for missing children and returning them to the unit or responding to aggressive behaviour and reports of damage to property. CSOs that have fostered good relationships with the local police report better understanding by police of the children's behaviours and improved responses.
Figure 2C shows the type of risk to residents and staff that can occur with a physically aggressive child in a unit.
Figure 2C
Example of extreme and challenging behaviour
|
One young person's behaviour included multiple examples of:
On average, an incident occurred every three days. |
Source: Victorian Auditor-General's Office based on a series of incident reports from one of the community service organisations visited during the audit.
Critical incident reporting system
The reporting process and information systems supporting DHS's category-based incident reporting system rely on manual data entry, which means that DHS cannot be assured that its response to critical incidents is efficient or timely.
The audit team observed the incident reporting system in practice and found it to be inefficient. CSOs are required to fax incident reports to a DHS divisional office, which then replicates this information into multiple databases.
Around 15–20 per cent of Category one incidents in OOHC are deemed to be abuse in care, defined as 'alleged or actual physical or sexual assault where a client in care is the victim and the perpetrator is either a carer, or a member of the carer's household'. An allegation of abuse in care triggers a quality of care review which includes investigation by a panel.
The audit examined quality of care reporting from 2010–11 to 2012–13. In 2010–11 there were 470 allegations of abuse in OOHC. The number of abuse allegations has increased. In 2012–13, the percentage of abuse allegations from residential care was 30.4 per cent of the total OOHC abuse in care allegations, yet residential care accounts for less than 10 per cent of the OOHC population. Of the allegations that were investigated and substantiated, 22 per cent were from residential care, and were for physical, emotional and sexual abuse.
Children who are at high risk
DHS has implemented a risk-based approach to actively monitor children who have been the subject of a high number of critical incidents. Children are placed on a high‑risk register and monitored closely. DHS divisions convene regular area-based meetings between child protection practitioners, local service providers and other relevant staff and professionals to coordinate service provision. The meetings enable problems and possible solutions to be discussed.
Examples of positive outcomes for some children on the register include better anger management, setting goals and planning for the future, reunification with family members, and better relationships with carers.
Another strategy to manage children who are at high risk is to place them in secure welfare services. There are two single sex secure welfare services in Victoria, each accommodating 10 children for a period of no more than 21 days. A lack of adequate accommodation is not by itself a sufficient reason for placing a child in a secure welfare service—the child has to be at substantial and immediate risk of harm.
Absconding and substance abuse are the two most common reasons for children being placed into secure welfare. For a child at substantial and immediate risk of harm, placement in a secure setting provides the only suitable option for ensuring the child's safety and wellbeing.
2.4 Stability
'I know that I can't live with my mum and dad but I would like to find a place that I can stay in forever rather than moving all the time and feeling more and more unhappy and not really understanding what's going on and why things keep changing, just as I get used to new people and a new place. I just want adults to see how hard it is for me not having one person in my life that really knows me, understands me and stays with me. This means adults keep making mistakes, getting confused, missing things and making me angry. Sometimes I get so angry that I explode like a volcano with no way of stopping until all the lava inside is out.'
– Robert, eight years old, residential care
Good practice: a statewide snapshot, DHS 2011
The best interests principles recognise the importance of continuity in the care of children. Children who experience multiple moves in OOHC have been found to be at risk of poor academic outcomes and mental health, with psychological and social harm more likely to occur after extended placement disruption.
Many children in residential care do not experience stability. A lack of placement options can lead to poor placement decision‑making and lack of staff continuity can reduce children's ability to form relationships and feel secure.
The Productivity Commission's Report on Government Services (ROGS) provides a benchmark, defining stability of placement as 'the proportion of children who had one or two placements during a period of continuous out-of-home care'.
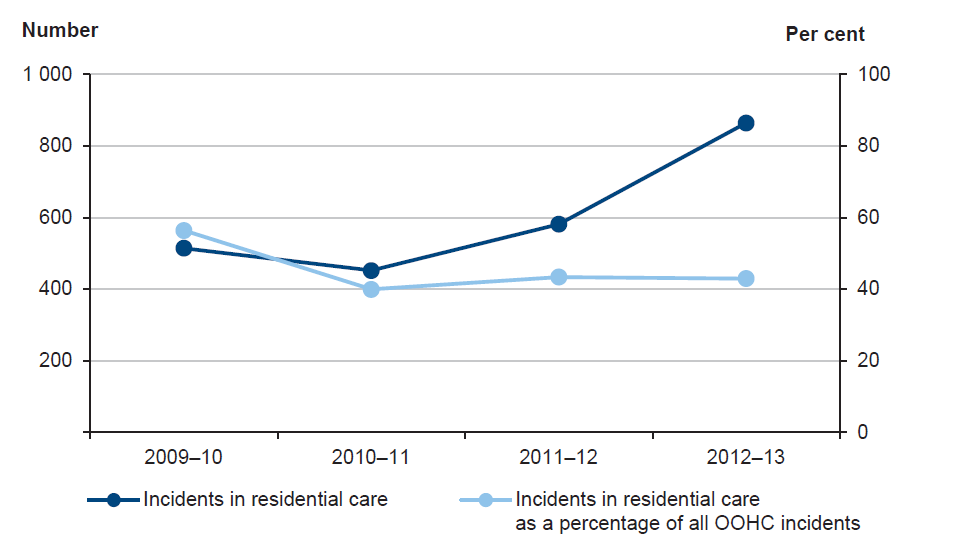
Figure 2D shows the number of placements experienced by children currently in residential care. Approximately one-third of children in residential care have experienced more than 10 placements and around 29 children have experienced 25 or more placements since entering the OOHC system. Placement disruption can also occur when there are failed attempts at reunification with family or failed placements with kinship or foster carers.
Figure 2D
Number of placements experienced
by children in residential care at June 2013
Source: Victorian Auditor-General's Office based on Department of Human Services Client Relationship Information System data.
In discussion groups and interviews with the audit team, DHS and CSO staff and young people in residential care reported that having a stable relationship and an established routine were also important elements of stability. Research highlights the importance of a nurturing relationship with a carer—even when young people have experienced placement disruption—in reducing the likelihood of further placement breakdown. Staff changes limit the opportunities to develop trusting relationships and establish routines.
2.5 Personal development
DHS has defined a range of personal development needs based on the best interests principles, including:
- achieving optimum health
- maintaining education
- maintaining family and cultural connections
- successfullytransitioning to adulthood after leaving care.
The lack of quality assurance mechanisms in place means that DHS cannot be confident that the personal development needs of children are being adequately planned for and effectively met. There is also no information about where improvements need to be made.
2.5.1 Inefficient systems and processes
DHS is responsible for developing case plans under section 167 of the Children, Youth and Families Act 2005. However, not all children have a case plan completed in the time frame required.
The case plan is based on conditions attached to the protection order decided by the Children's Court. The legislation requires that the case plan be reviewed annually. This review process helps to inform any subsequent court proceedings to extend the protection order. The development and review of case plans is the responsibility of DHS divisional staff.
In the 2009 Victorian Ombudsman report on the child protection program, the following recommendation was made:
Establish arrangements to ensure compliance with practice standards and key statutory obligations such as Best Interests Case Plans, Stability Plans and Cultural Support Plans. Ensure compliance is subject to independent scrutiny and regular auditing by an independent body and the outcomes of these audits are reported to Parliament.
In response to the Ombudsman's recommendation, DHS conducted a case file review of 1 714 files for children under new protection orders. The DHS file audit report highlighted the complexity of the client data system, with 78 per cent of the case files having to be reviewed manually.
The system operates as a depository rather than a Client Relationship Information System. Case plans were not where they should be in the system, often buried amongst hundreds of other documents. As reporting on compliance with legislative obligations relies on this data system, compliance reporting is not reliable.
CSOs reported being frustrated by the length of time taken by DHS to complete planning obligations. The audit examined DHS compliance reports and found that it has consistently failed to achieve this legislative requirement in the time frame required. At the end of June 2013, only 76.6 per cent of statutory case plans had been completed statewide within the six week time frame.
The audit conducted a case file review and found case plans and many other critical documents, such as individual education plans and care and transition plans, difficult to locate within the client information system. While the system has the capability to manage this requirement, it was evident that it was not being used to its potential, creating inefficiencies and waste. While some improvement could be made to the configuration, the primary issue is one of training and compliance.
Considering DHS has responsibility for these vulnerable children, the lack of an effective information system should be addressed as a priority.
2.5.2 Health
'I ended up pregnant. Had a prescription for the pill and had to ask every day for it from staff.'
– former resident
It is not possible to determine the overall health status of children in residential care due to the lack of trend and population data. The limited information available indicates that children in residential care experience poorer health outcomes, particularly in relation to mental health.
Young people in the audit discussion groups stated that drug and alcohol use was common among children in residential care and difficult to avoid. However, the extent to which these problems existed prior to a child being placed in residential care, or whether they began or increased while in care, is not known.
In 2012, DHS launched a Health and Education Assessment Initiative designed to comprehensively assess the needs of children entering or already in residential care, and to develop plans to address these. The initiative was allocated $12.8 million in the 2011–12 budget for a four-year period.
The health needs of a significant number of children in residential care are not assessed. In 2012, DHS conducted an audit to inform the rollout of the health assessment initiative and identified that:
- 28 per cent of children had not had a health assessment
- 20 per cent of children had no Medicare number on file
- 54 per cent of children had not had a dental assessment
- 57 per cent of children had not had a mental health assessment
- 71 per cent of children did not have an active general practitioner management plan.
Since the rollout of the initiative, there has been an increase in the number of appointments that children have kept with health professionals. In 2012–13, 62 per cent of children in residential care had at least one health contact under the health assessment initiative. In 2012–13, the health assessment initiative provided dental checks to 24 per cent of children in residential care, and initial health checks to 37 per cent and mental health assessments to 12 per cent of children in residential care.
This means almost 200 children did not receive any health assessments as part of the health and education assessment initiative in 2012–13. Figures for 2013–14 show an increase in the number of optometrist checks and general practitioner reviews compared to 2012–13. However, the number of audiologist (hearing) and optometrist (eyesight) checks provided remains low.
CSOs reported that children often have trouble keeping health appointments, mainly because of access to transport or anxiety. Having medical practitioners who understand the needs of children in residential care is therefore important. Having established this relationship through the initiative, it will be important for children to be able to maintain this relationship after leaving care. At this stage, the initiative does not extend beyond their time in care.
Figure 2E shows that children in TRC experience notable improvement in their health during their time in care, and for some time afterwards.
Figure 2E
Health outcomes for children and young people in
therapeutic residential care
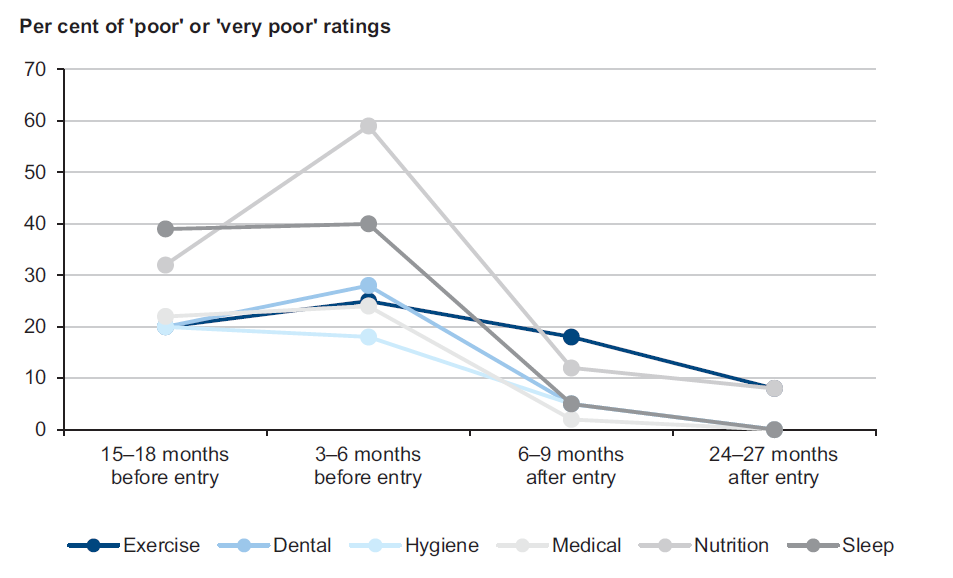
Source:Victorian Auditor-General's Office based on Department of Human Services therapeutic residential care evaluation 2011.
Prior to being placed in TRC, almost 40 per cent of children had difficulty sleeping. The number of children who slept poorly dropped dramatically after they had been in TRC for nine months.
In focus group discussions with young people who had recently left care, sleep disturbance was a significant issue due to fear associated with their current circumstances and past experiences of being unsafe.
2.5.3 Education
'Most kids in resi care do not go to school. It's hard to stay in school when you are moved too often; when you're with other kids who are not going to school—why would you go to school if the other kids aren't?'
– former resident
Educational outcomes for children in residential care continue to be poor. While enrolments have increased, the majority of children are not attending school regularly.
Education serves two key purposes for children in residential care. It provides them with stability through social interaction and a sense of community, and it also provides them with opportunities after leaving care through training and employment.
The education initiative, as part of a joint DHS and Department of Education and Early Childhood Development (DEECD) Health and Education Assessment Initiative, is progressing slowly. The first education assessment was in November 2012. As at July 2013, only 36 out of 460 planned education assessments had been completed, with the total number of assessments completed increasing to 188 by February 2014. Even adding in the 39 assessments that are currently in progress, this represents less than 50 per cent of the assessments that are due to be completed by 30 June 2014.
Education indicators show poorer results for those in residential care than in other OOHC placements. DHS data indicates that school enrolment levels for children in residential care have improved from 63 per cent in 2001 to 85.7 per cent in 2012. Children aged 13–17 years account for the majority of enrolments.
However, enrolment levels remain below the statewide levels of 100 per cent for primary school children and 87.6 per cent for secondary school children.
Figure 2F compares enrolment and attendance data from 2001 and 2012. While enrolments increased over this period, attendance remained stagnant, indicating that in these years fewer than 50 per cent of children in residential care attended school regularly. Figure 2G breaks down education characteristics by placement type.
Figure 2F
School enrolment and attendance among children in residential care
2001 |
2012 |
|
|---|---|---|
School enrolment |
63% |
85.7% |
School attendance (every day) |
48% |
49.3% |
Source: Victorian Auditor-General's Office based on unpublished data (2001) and unpublished Educational Characteristics Report 2012 (2013) from the Department of Human Services.
Figure 2G
Education characteristics by placement type, 2012
Residential care |
Other home based care |
|
|---|---|---|
Attend school five days a week |
49% |
88.% |
Attend school less than five days per week |
40% |
8.5% |
Suspended from school |
11.5% |
7.1% |
Expelled from school |
0.3% |
0.3% |
Source: Victorian Auditor-General's Office based on unpublished Educational Characteristics Report 2012 (2013) from the Department of Human Services.
A 2011 DHS-commissioned evaluation found that the TRC model had increased school contact and attendance, improved scholastic and language abilities and slowly improved academic functioning among children compared with data collected prior to their entry into TRC and compared to a control group of peers in the standard model of residential care.
2.5.4 Connection with family
'We will only be the state parent for 18 years, that's why we need to maintain engagement with the parents and family.'
– DHS
The best interests principles establish the importance of a child or young person remaining connected to their family. Discussions with residential care staff indicate a lack of capacity and capability to engage with the families of children in residential care. Of the CSOs visited as part of this audit, the TRC units showed greater integration of family into their models of care than those CSOs that provided standard residential care.
There is a shared responsibility between DHS and CSOs to make sure that staff have the capacity and capabilities to foster a positive connection between a child or young person and their family by engaging appropriately and effectively with families.
Connection to culture
'They do lose the cultural connection once they leave the community.'
– residential care worker
Development of a Cultural Support Plan is a legislative requirement under the Children, Youth and Families Act 2005 for each Aboriginal child in OOHC who is subject to a Guardianship to Secretary Order. While development of the plans has been outsourced to Aboriginal Community Controlled Organisations, the audit found that DHS does not actively monitor or report on compliance with this requirement. A recent DHS divisional audit to identify the level of compliance found that 81 per cent of children in OOHC did not have a Cultural Support Plan, which included children in residential care.
2.5.5 Leaving care
'We celebrate our 18th birthdays in the community, these kids fear them.'
– residential care worker
This fear was attributed by residential care workers to the fact that once a child has turned 18 and leaves residential care, they are on their own and do not necessarily have the skills or accommodation options to be able to live independently and safely. Figure 2H lists some of the everyday skills former residents in the focus group discussions identified as being needed.
Figure 2H
Required life skills identified by former residents
|
Children have varying experiences of being taught life skills in residential units. The focus group discussions with children formerly in residential care identified some of the life skills needed when leaving care, such as knowing how to:
These were considered to be 'normal', 'simple' skills that would equip young people to live independently. 'If I was at home mum would have taught me' one former resident said. |
Source:Victorian Auditor-General's Office.
In 2012, DHS produced Care and Transition Planning for Leaving Care in Victoria—a framework and guide to provide practitioners with 'best practice approaches', 'a strong developmentally based framework' for skills development, and 'a flexible, accessible service planning response that provides a bridge for young people from care to post‑care services, and to independence'. In 2013–14, DHS allocated $8.9 million to a suite of programs to support young people transitioning from care, or who have left care.
DHS does not monitor the development or implementation of transition plans for children in residential care. A 2010–11 DHS report found that only 63.7 per cent of children in residential care had the required care and placement plan on file, which for children over the age of 15 years, includes a transition plan. The case file review during the audit did not provide assurance that the level of completion has improved.
Support after care
'We prepare them for leaving care, take them up to the cliff edge and there's nowhere for them to go [after that].'
– residential care worker
CSOs report that support and accommodation options are limited for children leaving residential care. This is consistent with the 2011 DHS evaluation of the TRC model which found that 'the critical nature of exiting, exit planning and post exit support was raised by many CSOs as a subject of significant concern'.
Post-care destinations have included going home, living in shared accommodation, being offered a tent, staying with a friend, staying in a motel organised by a CSO, going into a lead tenant (semi‑independent) house, and staying in a two bedroom unit. A former resident who went home after leaving care advised that 'it's better to go to a place that you hate, for the bed.' In 2012–13, 409 children exited residential care. Figure 2I shows a breakdown of their post-care destinations. Of those who left residential care, 43 per cent returned to their parents or families.
Figure 2I
Destinations of children after residential care, 2012–13
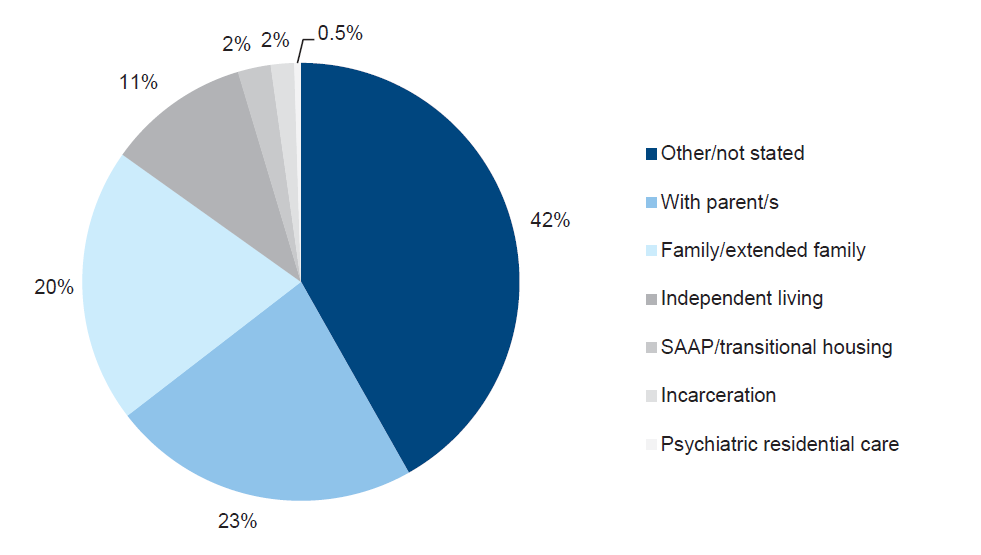
Note: SAAP refers to the Supported Accommodation Assistance Program. 'Other/not stated' includes 'unknown', 'no fixed address', 'whereabouts unknown' and the option of 'other', which is used if a child is exiting to an alternative location, such as moving interstate. Regardless of how 'not stated' is defined, it represents a significant proportion of children leaving care whose whereabouts is not specifically captured.
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services data.
2.5.6 Staffing capacity and capability
The effective and safe management of incidents in residential units requires skilled staff. However, there are no mandatory qualifications required to work in residential care services. Staff are employed to care for children with violent behaviours, mental health issues and often quite traumatic past experiences. A 2012 residential care workforce census found that 14 per cent of workers lasted less than six months in the job. In 2012, casual staff made up 55 per cent of the residential care workforce. The use of temporary staff can limit children's opportunities to develop a trusting relationship with a staff member and the use of inexperienced staff can lead to unsafe situations.
The audit found that the majority of service providers use a 'single parent' staffing model where one staff member works alone for most of the shift until handover at the change of shifts. This creates risks for both the child and the staff member, particularly in the event of a critical incident. The staffing model also makes it difficult for staff to make sure children get to school or to health appointments as staff cannot leave a child alone at the residential unit.
2.5.7 Independent advocacy in a child's best interests
Not all children in care know how to report an incident or who to report it to. Unlike children in other protective services, such as disability services, children in residential care do not have an independent advocate who looks out for them as individuals. This is particularly concerning given that these children have been removed from their families into care and most are under the custody or guardianship of the Secretary of DHS.
The audit team's visits to CSOs, and focus groups with young people who have recently left care, did not provide assurance that children knew the complaint-making process. Though the Charter for Children in Out-of-Home Care was displayed at all residential care services, it is not actively promoted by CSOs or DHS. While DHS has a central complaints process, it is not specific to children or the residential care system.
The audit found that there is nobody independent of DHS who has responsibility for hearing the complaints of individual children in residential care. The Commission for Children and Young People, for example, is not a complaints-hearing body. This raises the question of who will listen if the rights of children are not being protected.
Given that DHS is responsible for both managing the system and acting in the child's best interests, which may be in conflict with the system, there is an opportunity to create an independent role that would provide advocacy for these children.
2.6 Alternative models
A range of service and system adaptations have been designed to respond to the specific needs of children, including:
- a disability unit
- a house for young mothers
- a home for children under 12
- 'zipper units' which allow semi-independent living
- specialist two‑bedroom units
- single-sex units
- asibling house.
These alternative models of care allow a more flexible and responsive approach to particular groups of children who are less suited to standard residential care models. To have a sustainable system, DHS needs to be adaptive and identify where alternative models will provide maximum benefit and be an effective use of resources for particular cohorts of children.
Based on the children's stories captured in DHS's Sharing good practice, aspects of service provision that have made a difference to children's outcomes include:
- specialist assessments, therapeutic interventions, TRC
- proactive outreach to families, including parents, to establish or re-establish positive relationships with family
- one-on-one relationships and the development of trust between individual staff and children
- collaborationamong multiple service providers such as CSOs, child protection, schools and police.
More adaptive, innovative and flexible models could help improve outcomes for all children in residential care.
Recommendations
That the Department of Human Services:
- establishes alternative affordable models of care with sufficient flexibility to cater for the varying and complex needs of children
- actively promotes to children in residential care the processes for making a complaint and investigates the feasibility of establishing an independent advocacy role to support children in residential care
- develops performance measures for delivery of residential care services for children to meet legislative requirements and outcomes for children
- ensures that residential care staff have the necessary skills, qualifications, training and support to work effectively with children and their families
- identifies systems and processes for collecting and analysing information which better meet the department's compliance, assurance and reporting needs.
3 System design and planning
At a glance
Background
The effectiveness of residential care services relies on the capacity of the system to respond to the needs of children, the models of care available, and the cost of service provision. This Part looks at managing demand and capacity.
Conclusion
The residential care system is operating well over its funded capacity. Placements that have not been budgeted for generally lead to poorer outcomes for children. Strategies by the Department of Human Services (DHS) to divert children from residential care have had mixed success.
Findings
- In 2012–13, there was a 10 per cent shortfall between funded capacity and actual demand for placements.
- In 2011–12 and 2012–13, DHS had to purchase additional capacity to meet the demand for residential services at a total cost of $43.9 million.
- DHS relies on funding from other programs to meet the need for residential care services.
- Client complexity was the most expensive placement reason, with some placements costing close to $1 million.
Recommendation
That the Department of Human Services reviews existing demand forecasting approaches and develops plans for the capacity that is actually required.
3.1 Introduction
Most bed-based systems, such as hospitals and prisons, are not designed to operate at 100 per cent capacity. Some flexibility is necessary to accommodate additional people into the system and to allow for some movement of people already within the system.
The effectiveness of residential care services relies on the capacity of the system to respond to demand, the models of care available and the cost of service provision. To be responsive, the Department of Human Services (DHS) must be able to accurately and reliably forecast demand and be confident that there is sufficient capacity in the system to meet demand.
3.2 Conclusion
The residential care system is unable to respond effectively to the level of demand and the increasing complexity of children's needs. The system is operating significantly above its funded capacity. Operating over capacity can compromise placement decisions, lead to a reliance on additional funding, and reduce the opportunities for achieving quality outcomes for children. DHS is paying a premium to place children in residential care outside the planned capacity of the system.
Poor forecasting reduces DHS's ability to respond to growing demand, and DHS relies on funding from other programs to meet this demand.
3.3 Demand for residential care services
Demand for residential care is driven by a complex range of factors, including:
- the level of neglect and abuse in families
- decisions of the Children's Court, such as the number of Protection Orders issued
- availability of other placement options within the Out of Home Care (OOHC) system
- thesuccess or failure of programs that aim to divert children away from the OOHC system.
3.3.1 Current demand
Demand for residential care is currently outstripping supply. There are a number of drivers contributing to this, including the growing number of children entering the OOHC system, the capacity and effectiveness of home-based care options, and the length of time children are staying in residential care.
Distribution of services
The supply of residential care services is uneven across the state. Gaps in service delivery can result in poor placement decisions, with children sometimes being placed a significant distance from their family, school and friendship groups.
Profile of services
DHS has not mapped service providers by target group and location to determine whether the current services align with the needs of the children in those areas. The consequence of this is that children can be put in inappropriate placements, which may lead to placement breakdown and an increase in incidents.
Community service organisations (CSO) may provide residential care placement services across multiple DHS divisions. Figure 3A shows the profile of current residential care service provision.
Figure 3A
Profile of residential care population by division, 30 June 2013
|
Division |
Service providers |
Units |
Males |
Females |
Under 12 |
Mixed units |
Female units |
Male units |
|---|---|---|---|---|---|---|---|---|
|
North |
12 |
47 |
69 |
44 |
27 |
19 |
7 |
21 |
|
South |
9 |
53 |
83 |
64 |
14 |
27 |
8 |
18 |
|
East |
10 |
37 |
47 |
42 |
6 |
10 |
10 |
17 |
|
West |
9 |
54 |
94 |
61 |
18 |
21 |
12 |
21 |
|
Total |
40 |
191 |
293 |
211 |
65 |
77 |
37 |
77 |
Note: 'Unfunded placements' are included in this data. Units are residential units or houses.
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services data.
Based on the profile of residential care services:
- 40 per cent of residential care units currently house only males
- 19 per cent of residential care units currently house only females, yet females accounted for 42 per cent of the residential care population.
The audit identified that 60 per cent of CSOs have children aged under 12 years in their care.
Planning for services needs to be informed by the staffing capability and funding mix agreed with service providers, and the age and complexity of the children involved. Where providers have specialised skills in particular models of care, these providers should be the preferred option for a child in need of those specialised skills.
3.3.2 Forecasting demand
DHS uses three year forecasts of the number of OOHC placements needed in order to secure additional funding from the Budget and Expenditure Review Committee. Ten year forecasts are used in longer-term planning. Forecasts are therefore used strategically rather than operationally.
DHS uses the daily average occupancy of residential care services to project future demand. Based on daily average occupancy figures since July 2011, the level of demand has consistently been above the funded placement level in every DHS division every month.
The audit examined documents submitted by DHS to government over the past five years as part of the budget process and found that DHS has alerted government to the pressures on residential care services during this period.
In 2008, DHS reported a $14 million budget deficit due to several pressures:
- In the past 10 years, demand for OOHC services had increased by 50 per cent.
- Children were spending longer in residential care.
- Demand for residential care was outstripping supply, and children were being accommodated in temporary and unsuitable emergency placements such as motels and caravan parks.
- The level of demand was increasing at a time when the number of foster carers available in Victoria was declining.
By 2011–12, the budget deficit had escalated, prompting a review of DHS base funding—in particular, the delivery and financial performance of OOHC. The review found that the deficit was largely due to residential care placement services.
Demand forecast monitoring
DHS is reliant on successful Budget submissions to meet its legislative obligation to place children in OOHC.
The 2010 Victorian Ombudsman's report into OOHC recommended the development of models for projecting future resource demands for the OOHC system 'that provide greater opportunities for ensuring demand is met through planned capacity increases rather than ad hoc arrangements'.
Based on DHS residential care demand projections, the number of placements required is expected to increase by 29 per cent from 2012–13 to 2017–18.
Figure 3B
Department of Human Services projections for residential care to 2017–18
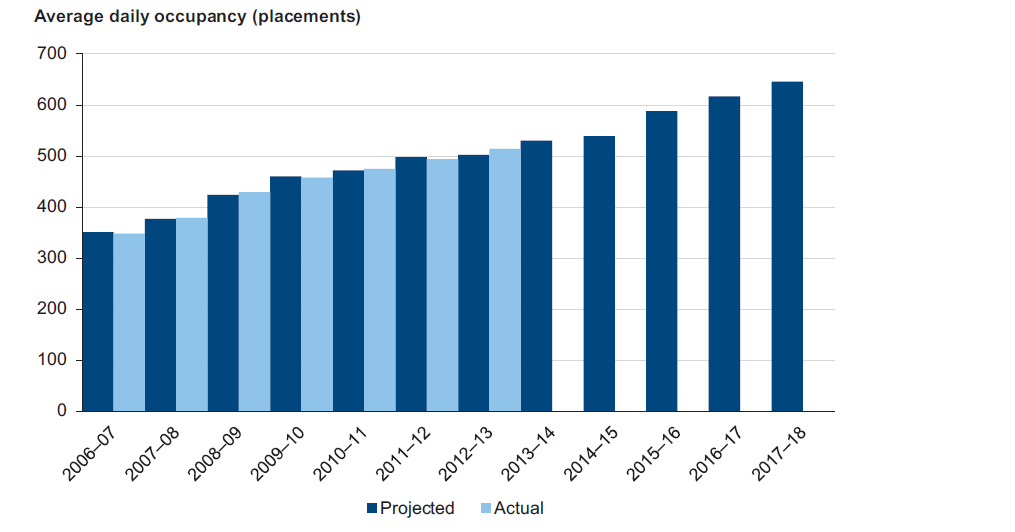
Source: Victorian Auditor-General's Office based on Department of Human Services unpublished data.
Figure 3B shows that DHS expects a steady increase in placement demand.
Demand for residential care is reported to the DHS board through monthly Performance, Assurance and Compliance (PAC) reports. However, these reports do not enable assessment of DHS's capacity to meet forecast demand projections as they do not track actual demand versus forecast demand, or actual demand versus actual funded capacity now or into the future. This lack of transparency limits the ability of the DHS board to respond to the level of demand through planned capacity increases, have confidence that strategies in place to manage demand are working or redirect effort to where it is needed most.
3.3.3 Diversion strategies
The preference of the government over the past five years has been for DHS to develop diversion strategies to contain demand.
There have been mixed results from DHS's diversion strategies. One successful outcome has been to gradually reduce the proportion of children in residential care who are under 12 years of age. However, this means there is now a larger proportion of adolescents in care, with more complex behaviours, who are less likely to be transitioned to home-based care places and are staying longer in residential care. As more adolescents are placed in care now than previously, the system needs to identify better ways to respond.
3.4 Service capacity
Capacity is the maximum level of services that can be provided within available resources, such as funding, staffing and floor space.
There is insufficient funded capacity in residential care to meet demand.
3.4.1 Current service capacity
DHS routinely places children in residential care placements that do not meet the child's level of complexity. Inappropriate placements, based on bed availability rather than on matching the needs of a child with the needs of children already in a unit, was one of the most common issues raised by CSOs during the audit.
Service agreements
DHS funds CSOs through funded service agreements to deliver residential care placement services to children. These agreements set out the key obligations, objectives, rights and responsibilities of the parties. CSOs report against three performance indicators:
- daily average number of placements
- percentage of children subject to protective involvement
- totalnumber of planned exits.
The performance indicators focus largely on throughput and are intended to measure the achievement of service objectives, not the outcomes for children.
The number of funded placements in the service agreements sets the limit of capacity for DHS and is a measure of supply. In 2012–13 the total funded capacity of residential care was 459 places. This includes fixed-term—typically less than 12 months' duration—and ongoing places.
At the start of 2012–13, DHS planned for residential care funded capacity of 370 placements, and over the financial year entered into fixed-term funding arrangements with CSOs to provide an additional 89 fixed-term funded placements. These fixed-term placements are time limited and may be used for children who are engaged in transition planning for reunification with their family, placement in home-based care or leaving care for independent living.
Figure 3C shows the distribution of total funded capacity in 2012–13. This distribution is based on the previous DHS regional structure, and shows that the North and West Metropolitan region had the most funded residential care placements in 2012–13.
Figure 3C
Residential care total funded capacity by region 2012–13
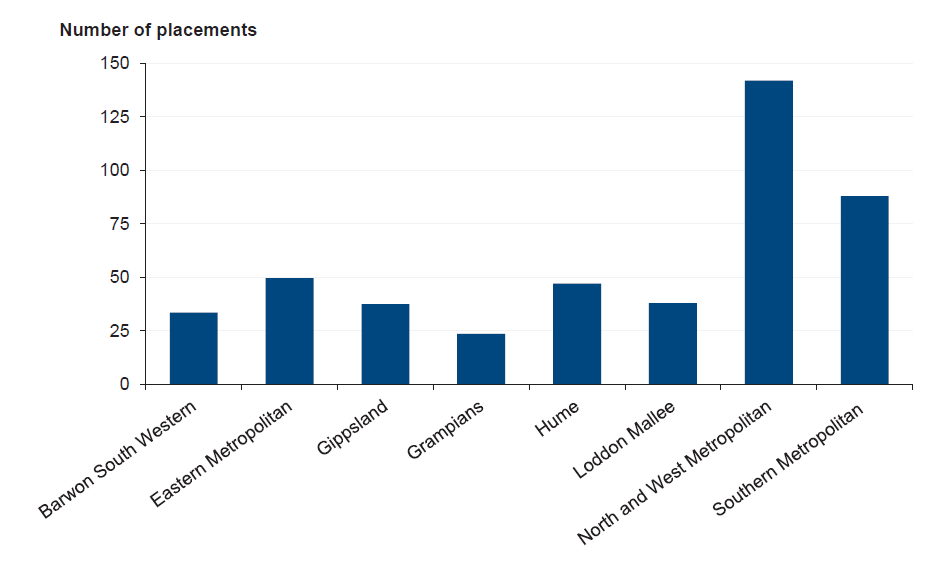
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services data.
CSOs are funded by DHS on a client mix basis of either intermediate or complex needs. Intermediate placements cost $162 880 per year or $446 per day. Complex placements cost $233 448 per year or $639 per day. The higher level of funding is provided to CSOs that can provide a placement service to a child with more complex needs.
Figure 3D
Funded placements by client need, 2012–13
|
Division |
Intermediate |
Complex |
|---|---|---|
|
Barwon South West |
13 |
20 |
|
Gippsland |
16 |
21 |
|
Grampians |
17 |
7 |
|
Hume |
23 |
24 |
|
Loddon Mallee |
14 |
24 |
|
Eastern Metropolitan |
35 |
15 |
|
Southern Metropolitan |
52 |
36 |
|
North and West Metropolitan |
47 |
95 |
|
Total |
217 |
242 |
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services data.
Figure 3D shows the breakdown of total funded placements by client need across the previous DHS regions. These figures include 49 intermediate and 41 complex placements which had fixed-term funding. They also include 72 therapeutic care placements. Thirty-five intermediate and 37 complex placements received a loading for the provision of therapeutic residential care (TRC) services. In 2013–14, the TRC loading provides an extra $74 580 per placement for additional supports, such as a therapeutic specialist and additional staff. This means that a complex placement with TRC would cost $308 028 per year or $843 per day.
Figure 3E shows the breakdown of expenses for the provision of care to four children in a complex residential care placement.
Figure 3E
Complex care expenses, 2013
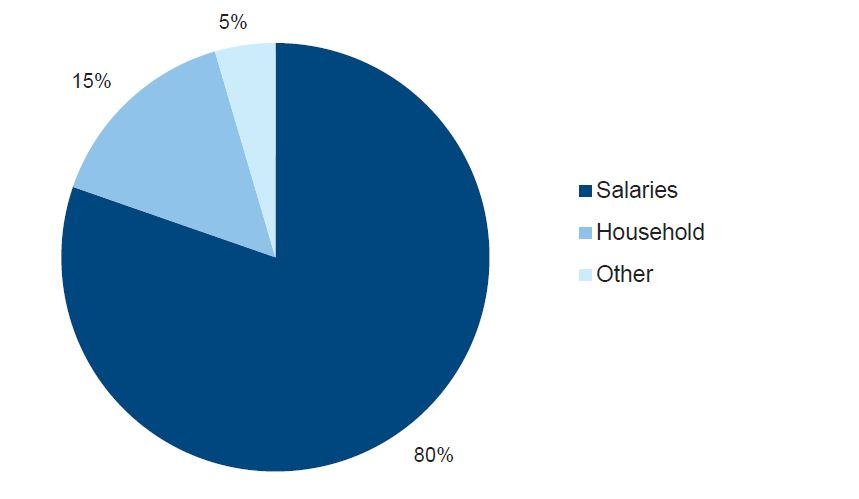
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services documents.
Eighty per cent of the funding for complex residential care is for staffing expenses—salaries, shift allowances and on-costs—with the remainder for household expenses—food, clothing, power, medical, personal care and entertainment—and other expenses, such as staff training. On a per hour basis, the cost to provide these services in a unit accommodating four children is around $106 per hour, or $26 per hour per child. By comparison, intermediate care costs $18 per hour per child, with the TRC loading adding $8.50 per hour per child where applicable.
By comparison, youth justice services cost $22 per hour per child, disability respite costs $21 per hour per child, and therapeutic foster carers are reimbursed $2.82 per hour per child.
In total, residential care funded placements cost around $100 million per year to provide.
Figure 3F depicts the level of supply versus demand. Supply is the total funded capacity (ongoing and fixed-term funded placements) against the level of actual demand (monthly daily average occupancy) for 2012–13. The annual daily average occupancy for 2012–13 was 508 placements (excluding secure welfare service placements). This means on any given day an average of 508 children were in a residential care placement.
Figure 3F
Supply versus demand for placements, 2012–13
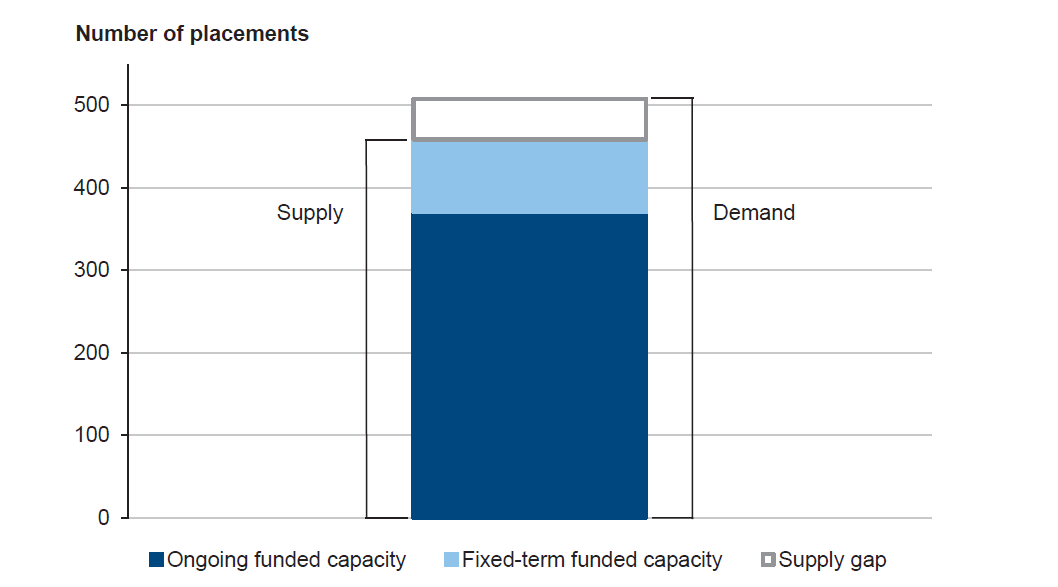
Note: As the Department of Human Services places all children, there is no unmet demand.
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services data.
Figure 3F shows that there is insufficient funded capacity to meet actual demand for placements. There is a 27 per cent gap between ongoing funded capacity and actual demand for placement. This capacity shortfall has been further reduced by funding additional fixed-term placements on a short-term basis. However, even with this additional funding, a capacity shortfall of 10 per cent remains.
DHS must ensure that it can provide placements to children in need of residential care as this is a statutory responsibility. To do this, DHS relies on additional purchased capacity or contingency places known as 'unfunded placements'.
3.4.2 Purchasing additional capacity
DHS funds the shortfall between funded capacity and demand from other areas outside the residential care budget.
To manage the lack of capacity DHS has had to purchase additional capacity. This purchasing behaviour was the subject of the recent DHS base funding review, which identified that unfunded placements were the major cause of the DHS budget deficit.
Cost shifting
In 2011–12, DHS purchased $11.3 million additional capacity through cost shifting—see Figure 3G.
Figure 3G
Funding sourced from other Department of Human Services activities
|
Funded activity |
Amount ($mil) |
|---|---|
|
Health and Education Assessment Initiative |
3.4 |
|
Building the Capacity of Aboriginal Organisations |
1.0 |
|
Investing in a Better Future – Leaving Care Initiative |
2.8 |
|
Cradle to Kinder Program |
1.0 |
|
Disability Services Respite Program |
1.4 |
|
Disability Services – Training backfill funding |
0.5 |
|
Disability Services – Mental health contingent funding |
0.9 |
|
Development of family violence risk assessment tools |
0.3 |
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services data.
CSOs refer to an unfunded placement as a 'planned placement', arguing that the lack of capacity is not always about physical space, but the lack of sufficient models of care to meet the needs of children within the funded placement system. From a risk management perspective some children are better placed within a one-to-one model—that is, one child in one unit with at least one, but often more, staff in attendance. Some CSOs argue that the funded placement amount does not provide sufficient resources to keep the children safe.
The use of unfunded placements has stalled the implementation of other programs designed to improve the quality of services within OOHC and other DHS program areas. For example, the lack of preparation given to children prior to leaving residential care has been identified as a problem by CSOs, yet $2.8 million has been taken from the Investing in a Better Future – Leaving Care Initiative to fund additional unfunded placements.
Reasons for purchasing additional capacity
The main reasons for purchasing additional capacity are demand, client complexity, and the desire to keep a sibling group together.
Figure 3H shows the number of unfunded placements that were purchased in 2011–12 and 2012–13 based on the reason recorded. In three of the four DHS divisions, demand was the most common reason given.
Figure 3H
Reason for placements outside funded capacity by division, 2011–13
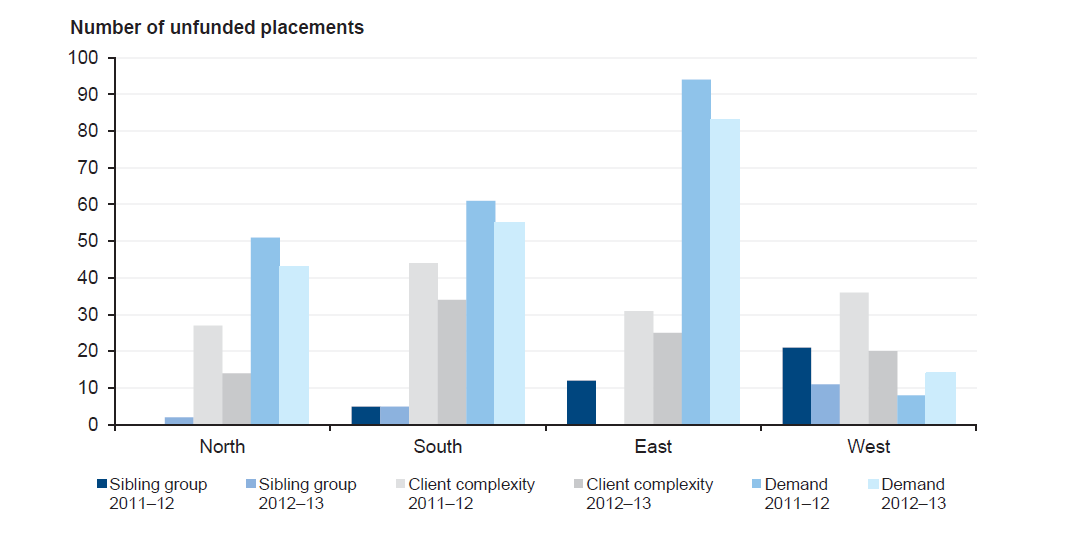
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services data.
The audit found that East division purchased the most unfunded placements due to demand in both years. East division also had the least funded places, which may explain the higher utilisation of unfunded placements. By comparison, West division purchased more unfunded placements because of client complexity.
Figure 3I
Unfunded placements by client complexity issue
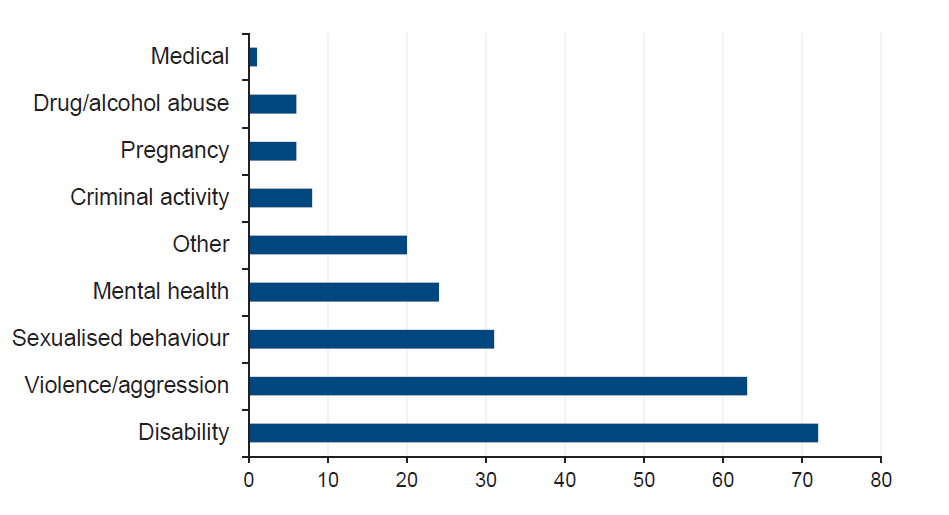
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services data.
Unfunded placements for client complexity reasons provide an individualised response. Figure 3I shows the number of children in unfunded placements by complexity issue. As shown, disability and violent behaviour are the most common issues funded.
The cost of purchasing additional capacity
CSOs are required to submit a proposal to DHS for placements outside their existing capacity. DHS needs to examine the criteria for accepting an unfunded placement proposal, with a view to setting limitations on cost and expectations on delivery.
The need for additional funds to provide services may indicate a CSO's lack of capability to provide these services. DHS should examine the reasons for unfunded placements to identify if other assistance could be provided to CSOs to enable them to manage complexity within the funded system.
CSOs present DHS with an unfunded placement costing. An examination of these costs identified significant differences in the cost of service provision between CSOs, with CSOs charging a premium for supervision services to monitor the predominantly unqualified staff employed to care for the child. There are no economies of scale in these agreements, and no evidence of DHS recouping any advanced funding when an available funded placement, deemed unsuitable, has not been used. In many instances the child is placed within an existing funded unit, meaning the actual cost of service provision is more.
In addition to the cost of purchasing additional capacity, DHS has an obligation to make sure that any property used for a placement meets regulatory requirements, including fire safety requirements. To meet lease payments and make the properties fit for purpose, DHS spends around $60 000 on each property over a 12-month period. These costs do not form part of the CSO proposal. Currently around 40 properties are leased by DHS to provide unfunded placements.
In an effort to reduce the use of private lease arrangements for additional placements, $9.1 million was provided in 2012–13 to improve capacity through the construction of eight new residential care units. Construction is due to begin in 2014–15.
DHS purchases additional capacity at a premium. On a daily cost basis, unfunded placements due to client complexity significantly exceed all other residential care placements, including the most expensive standard residential care option available.
In total, 390 extra unfunded placements were purchased in 2011–12 at a cost of $19.9 million, and 306 places were purchased in 2012–13 at a cost of $24 million. Client complexity was the most expensive placement reason, with some placements costing close to $1 million. By contrast, demand was the least costly placement reason, being shorter in duration and costing less on a daily basis to provide.
Figure 3J shows the cost comparison between funded and purchased capacity (unfunded) places.
Figure 3J
Cost of residential care service provision, 2012–13
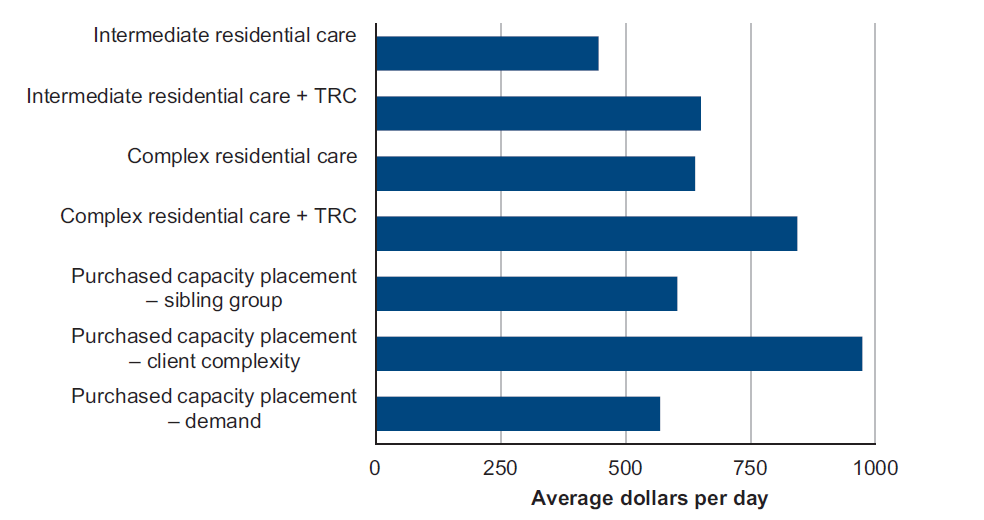
Note: A TRC loading is applied to an existing funded placement to provide additional support.
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services data.
The audit found that client complexity placements were less likely to be short term.
Cost efficiency
Purchasing additional capacity is expensive, inefficient and unsustainable. High cost unfunded placements are putting pressure on the system and DHS needs to identify whether these services could be more efficiently provided within funded capacity or through more specialised responses.
Based on the unfunded placement data provided for 2011–12 and 2012–13:
- 397 individual children received 696 placements
- 27 per cent of children received 79 per cent of unfunded placement funds—$34.9million
- 73 per cent of individual children were placed using only 21 per cent of funds—$8.9million
- 119 placements cost more than $1 000 per night
- 3 per cent of placements cost $7.9 million.
Figure 3K shows the unequal distribution of funding to individual children over the two‑year period.
Figure 3K
Distribution of funds across unfunded placements, 2011–13
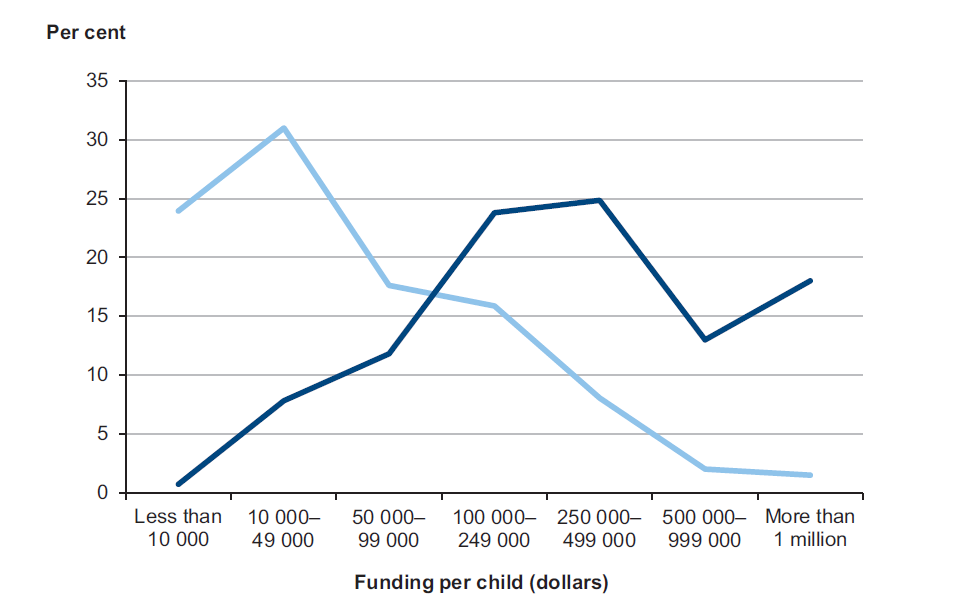
Source: Victorian Auditor-General's Office based on unpublished Department of Human Services data.
Fourteen individual children received placements costing more than $500 000 due to client complexity. DHS needs to plan for and identify more efficient ways of arranging placements for children with complex needs.
Figure 3L shows a breakdown of the expenses incurred in an unfunded placement that exceeded $500 000. This placement for one child cost $186 per hour to provide.
Figure 3L
Example of unfunded placement expenses
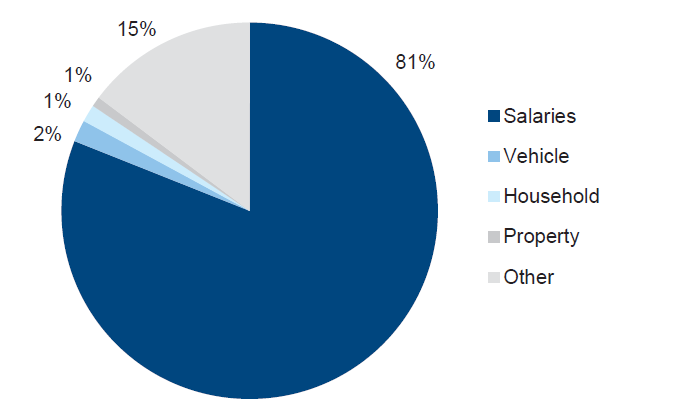
Source: Victorian Auditor-General's Office based on Department of Human Services sample of Community Service Organisation unfunded placement costings, 2013.
Figure 3L shows that salaries account for 81 per cent of the total expenses calculated, similar to the proportion of expenses in funded placements. However, the actual amount claimed was double the amount of an equivalent funded placement. If this example, which was costed for a six-month period, was for a full year, the total cost would have been in excess of $1.5 million.
The audit found examples of CSOs receiving more funding to deliver unfunded placements than for funded placements. These arrangements have the potential to create a reliance risk for DHS as CSOs may factor these payments into their budgets.
Under-utilised capacity
During site visits the audit found that some units have available capacity. While DHS has purchased additional capacity using funds from outside the residential care budget, there is also evidence to confirm that DHS has approved a reduction in capacity in some circumstances.
The case study in Figure 3M is an example of where DHS has agreed to cap the capacity of a residential care unit.
Figure 3M
Case study – capping capacity
|
In one DHS division two children with extremely high needs and aggressive behaviours were on their own in two separate residential care placements. One was a funded placement and one was an unfunded placement. Due to the higher costs of unfunded placements, and the under-utilisation of capacity in the funded property, a decision was made to move the children in together. As the combined risk of behaviours posed an increased threat to both children and staff, DHS made the decision to cap the capacity of the funded house from four to two. Additional staffing was provided to manage the increased risk, and to provide a higher level of supervision for the children, during transition and beyond. |
Source: Victorian Auditor-General's Office based on Department of Human Services data.
DHS is unable to readily recoup or redirect funding in instances where placement capacity is not used for operational reasons.
DHS does not make sure that agreed funded placements are taken into consideration when placement capacity is purchased. The audit identified that some CSOs are rejecting placements while still receiving agreed funding to provide services in the future. This situation is untenable if residential care is to remain sustainable and DHS is to fulfil its statutory responsibilities for children in its care.
Recommendation
- That the Department of Human Services reviews existing demand forecasting approaches and develops plans for the capacity that is actually required.
Appendix A. Audit Act 1994 section 16—submissions and comments
Introduction
In accordance with section 16(3) of the Audit Act 1994, a copy of this report was provided to the Department of Human Services.
The submissions and comments provided are not subject to audit nor the evidentiary standards required to reach an audit conclusion. Responsibility for the accuracy, fairness and balance of those comments rests solely with the agency head.